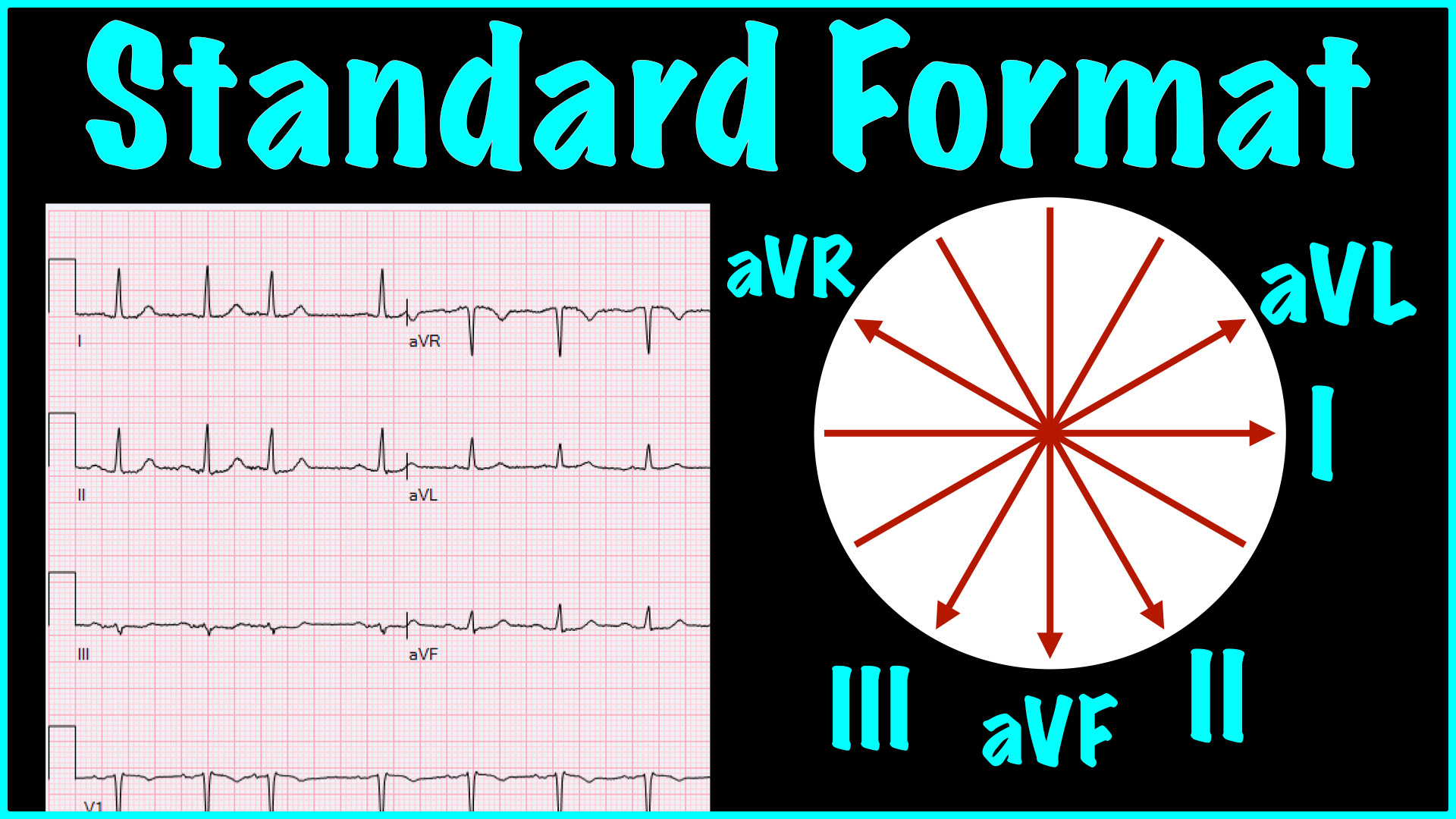
On a standard EKG, the precordial leads (V1-V6) are presented in an “anatomically contiguous” manner. That is not the case with limb leads. The Cabrera format is way to rearrange the limb leads on the printed electrocardiogram such that they ARE in an “anatomically contiguous” arrangement.
Putting the limb leads in the following order: aVL, I, -aVR, II, aVF, III puts them on paper in an “anatomically contiguous” arrangement.
I suspect dogma is the only thing keeping this from being standard. Once you understand it, it is difficult to make a compelling case for the classic arrangement of the limb leads on the electrocardiogram.
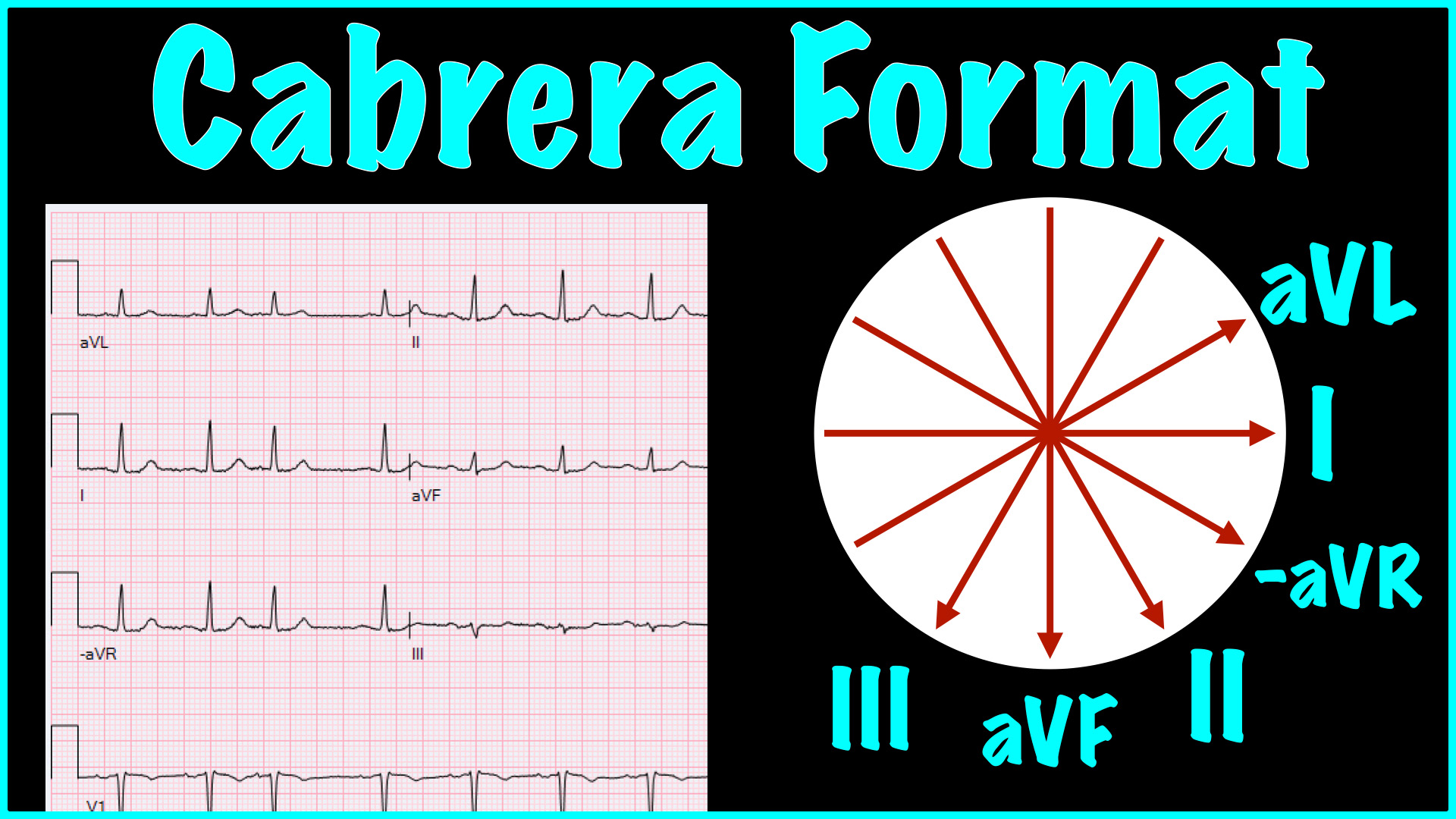
Turning aVR upside down gives us “-aVR”, which anatomically is located between leads I and II. That swap allows the leads to be displayed in way that puts them in an “anatomically contiguous” layout.
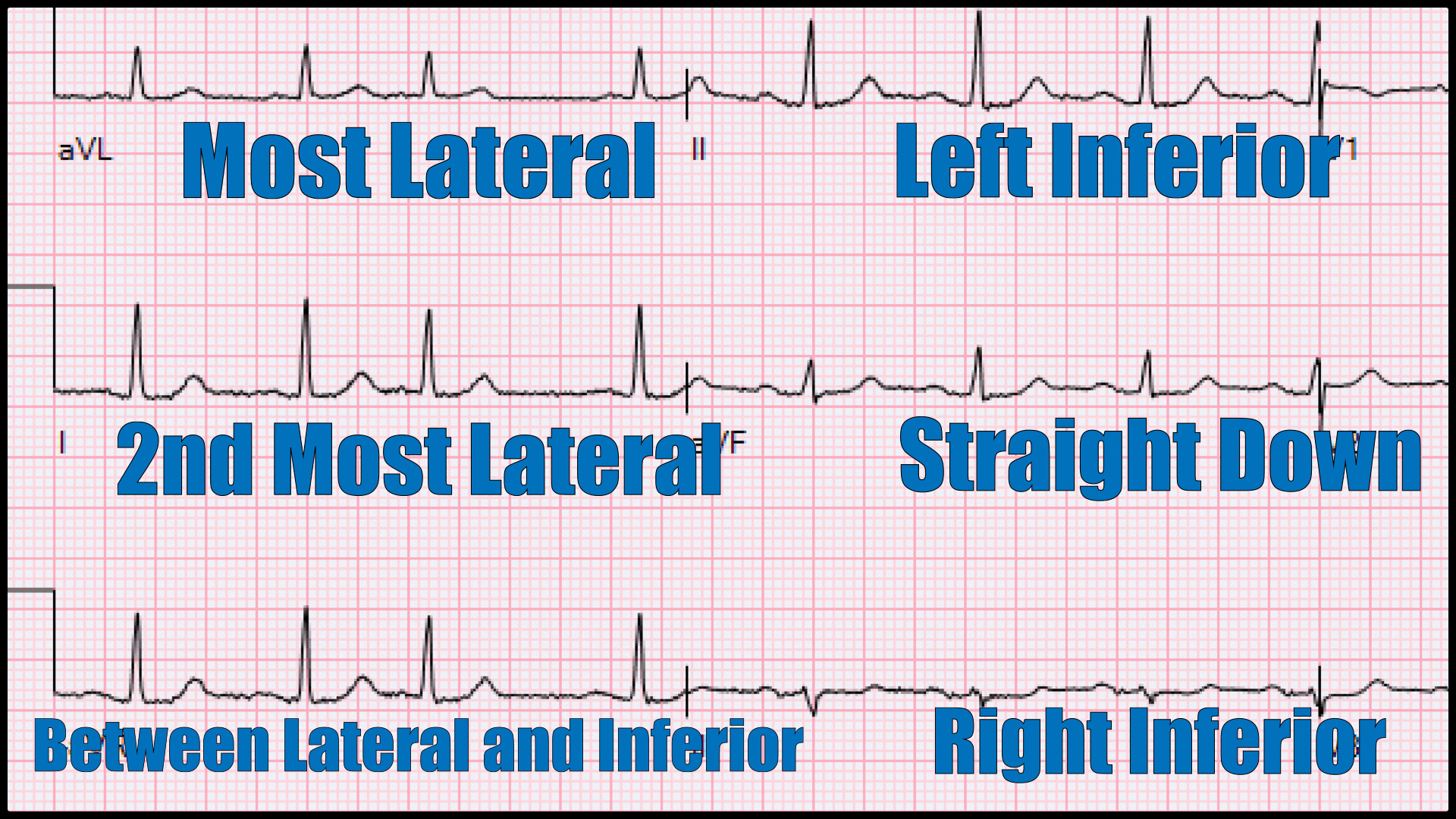
This format makes determing the axis more intuitive. Also, the diagnosis of an ST-elevation myocardial infarction requires elevation in “anatomically contiguous” leads. This format makes those relationships obvious, rather than having us memorize which leads are “inferior” or “lateral”.
It may not be earth-shattering, but it is great thought experiment. Your EKG machine and/or archive software can probably display in this format if you dig deep enough into the settings.
