A man slipped on the ice and hurt his right chest wall. The radiologist says there are no fractures. I’m still suspicious. Is there a better a way?
We could do a CT scan, but that feels like overkill given the “normal” rib X-rays.
How about an ultrasound?
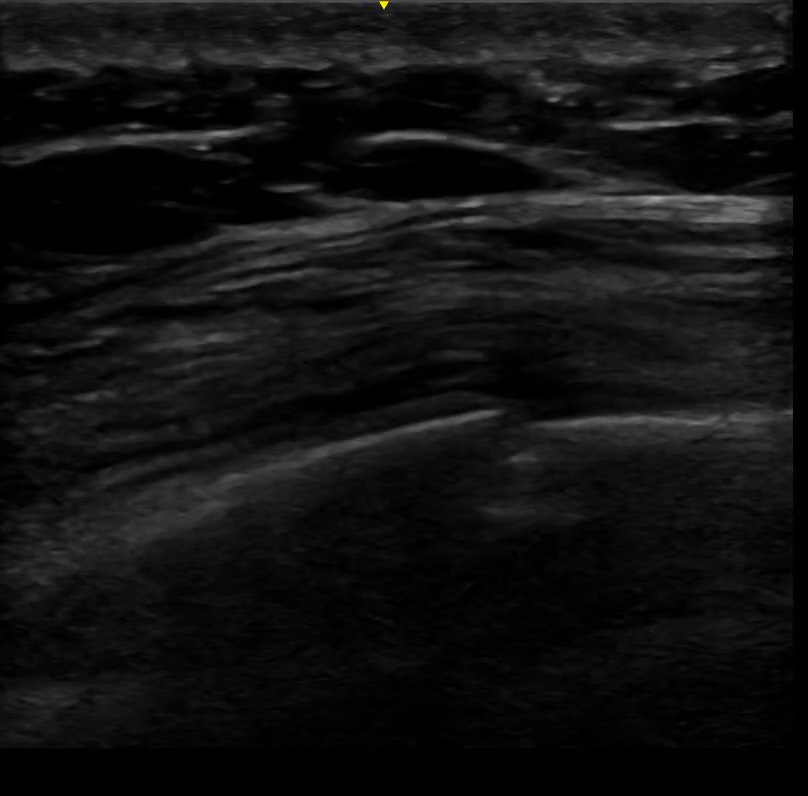
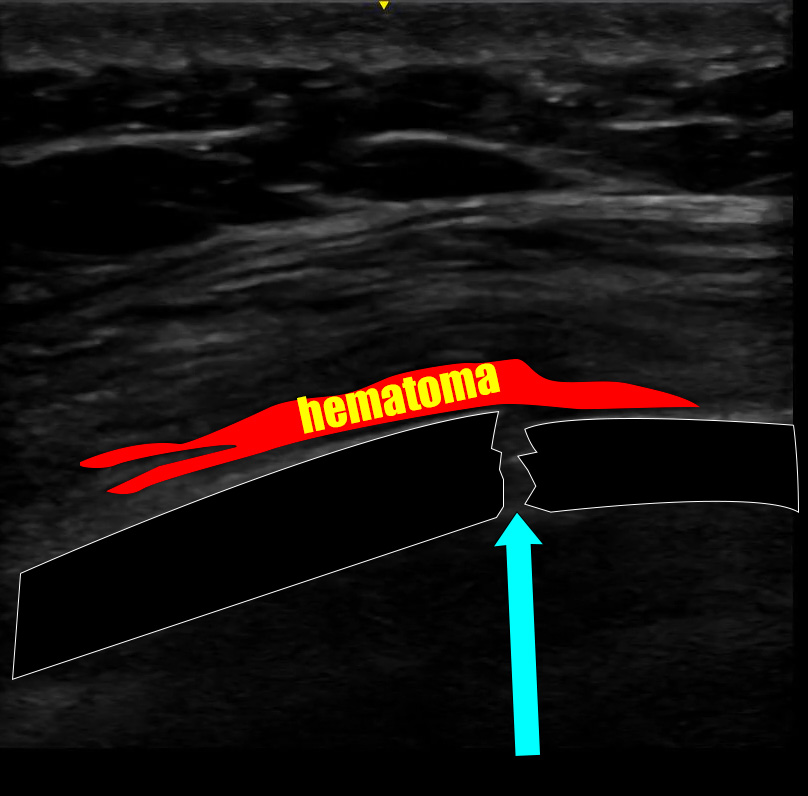
We clearly see a rib fracture here.
It is unreasonable to think that you might trace the entire length of every rib from the spine all the way around the chest wall to look for rib fractures. It would take forever and some portions of the ribs are hidden by the scapula and clavicle. So, a “comprehensive” ultrasound to definitively rule out rib fractures probably is not a realistic use of time.
However, the beauty of the ultrasound is that you can ask the patient to point with one finger to where they hurt the most. If they can find a pinpoint location, that’s where the fracture is going to be. It can be used in a very focused manner: localize the pain, then trace the rib in long axis with a linear transducer in that area. It would be wise to also look at a rib or two above and below the one they point at.
Is ultrasound the best test in every situation to look for rib fractures? Of course not. But, in the right patient, it is very easy to see a broken rib on ultrasound.
Could one argue the point that as long as there is no pneumothorax, flail segment, or grossly displaced fractures that it does not really matter if there is a subtle, non-displaced rib fracture? Sure. But, we all know that the patients like to know if their bones are broken. You look like a hero if you can show them fractures on the ultrasound screen that the X-ray missed. It provides some diagnostic closure for them as well, and the extra face time with a thorough provider is always a crowd-pleaser. The patient described above was actually a bounce back. He got the X-ray at the initial visit, but a few days later couldn’t understand why he was still hurting so badly if his bones weren’t broken. It just took a minute to find that the rib actually was broken – two in fact. He was relieved at the diagnostic closure and prognostication, even if the rib still hurt.
Finding rib fractures on ultrasound also opens the door to a costal nerve block, if you were so inclined. Again, there are arguments to limitations of the procedure, but if you’ve ever seen the total relief a patient gets from numbing up a single rib fracture you’d consider it.
Pitfalls?
- Assuming the fracture you see is the only one, which could lead you to miss multiple fractures or even a flail segment. You have to be thorough – especially if there was not an x-ray done.
- Seeing the junction where rib meets costal cartilage and mistakenly thinking you are seeing a fracture
- Not looking for lung sliding at the apex to make sure there is no associated pneumothorax
Scan happy, my friends

Good read, Dr. Steele! When would you consider an ESP block over intercostal? Does the risk of pneumo make it more preferential to perform an ESP block instead?
LikeLike
Intercostal is great when there is only one fractured rib. It wouldn’t make sense to block one rib if several were broken. Also, people tolerate the pain of broken rib very differently. Mot don’t need this procedure. But, in the right person, ultrasound localization is fantastic in this case. You see the fracture, mark the rib with a pen, follow the rib with the ultrasound until you are posterior to the fracture (proximal in terms of the innervating nerve) and put local anesthetic right under it. It’s a small volume of anesthetic and works like a charm. You do have to have fantastic “needle discipline” during the procedure because you are right on the pleura. But assuming you have developed that skill with vascular access and less risky nerve blocks (medians, ulnars, etc) then this is an obtainable skill for an ED provider.
ESP on the other hand would be better if there were multiple fractures – especially posterior rib fractures. ESP blocks look easy in demonstration videos, but in my experience the patients often have a body habitus that is problematic and may have trouble getting into a good position for the procedure with multiple rib fractures. So, it’s a great option, but there are a few potential hurdles. One upside is that there is no pleura nearby, so the risk of pneumothorax is not there.
Serratus plane blocks are another option for multiple rib fractures, especially if they are lateral or anterior. I don’t think it would help much “upstream” from the block, which is placed laterally on the chest wall.
LikeLike