Part two in our three part series on bladder ultrasound. We will look at two cases.
Case 2
A 64 year-old man presents with complaints of urinary frequency and the feeling of incomplete bladder emptying for a month or so. His exam was benign. The case seemed cut and dried: urinary tract infection vs benign prostatic hypertrophy. The urinalysis was clean, so BPH seemed to be the most likely diagnosis. He insisted that he still felt full even after giving the urine sample, so we decided to have a look to see how full he was. Frankly, I was expecting to use the ultrasound to decide whether or not he might benefit symptomatically from a catheter. However, this is what the images showed:

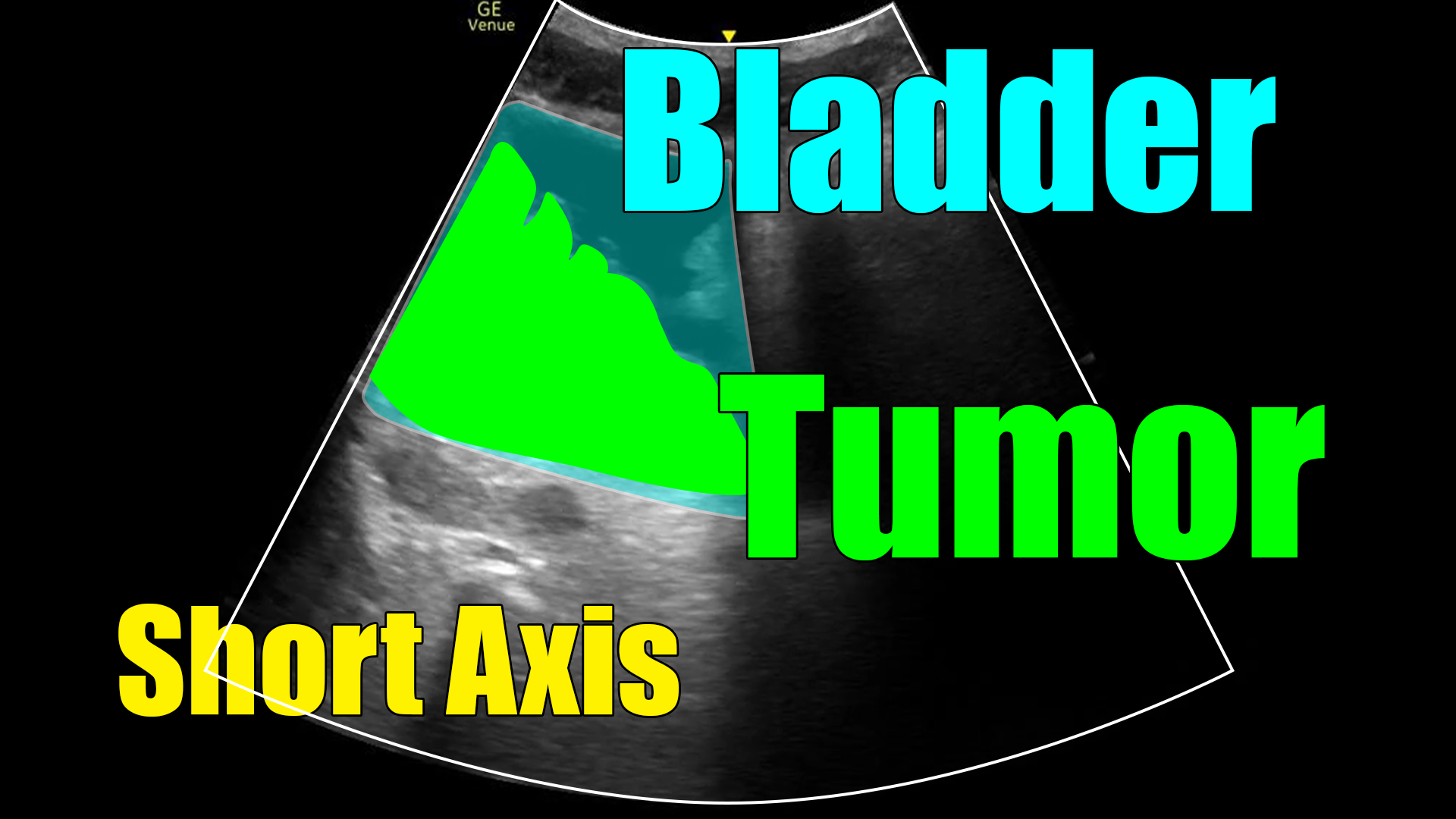
What we are seeing here is cancer. Hematoma or clot is on the differential as well, but notice how this is oddly shaped and adherent to the wall of the bladder? A clot, which generally has the consistency of a thick liquid or gel, would more likely be shaped like the rounded walls of the bladder and be mobile. So, although not “diagnostic” of cancer (at least in my hands), this is very concerning.
This scan probably expedited his diagnosis by several weeks – maybe more. It might have been tempting to try tamsulosin and refer him back to his PCP. A PSA would probably have been checked at follow up, but who knows when that would have been and it may or may not have been elevated with bladder cancer. Maybe he gets further imaging, and maybe he gets urology referral. Or maybe they try the tamsulosin for a few months if the PSA is not elevated. Again, in an outpatient setting those things may take a while.
Case 3
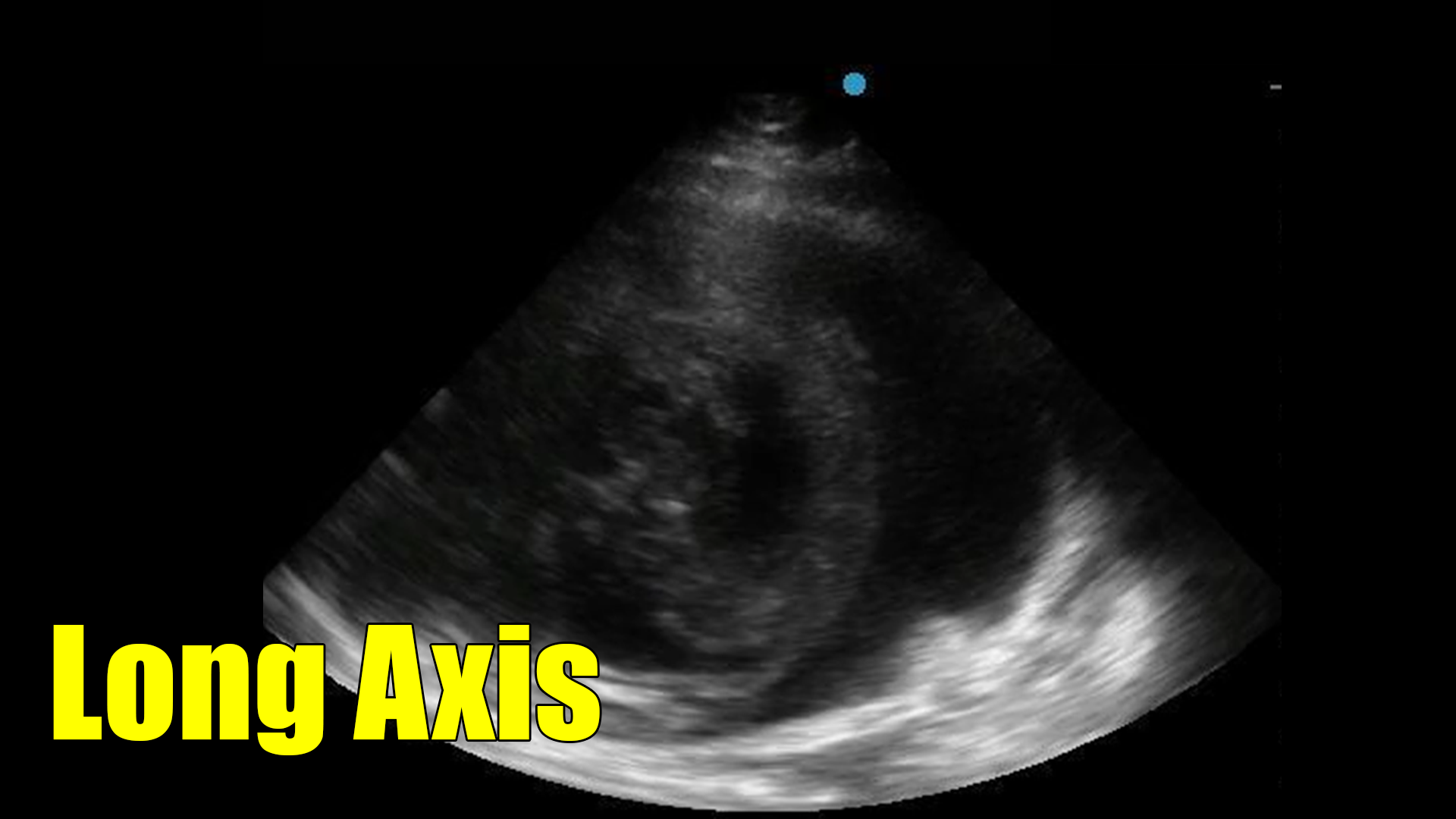
A 72 year-old lady presents for evaluation of one day of urinary retention. A Foley catheter was placed, but only blood and blood clots came out. As we saw in the previous post, this scenario should raise concerns for the balloon not being in the bladder. So, we took a look with the ultrasound. Here are the images.
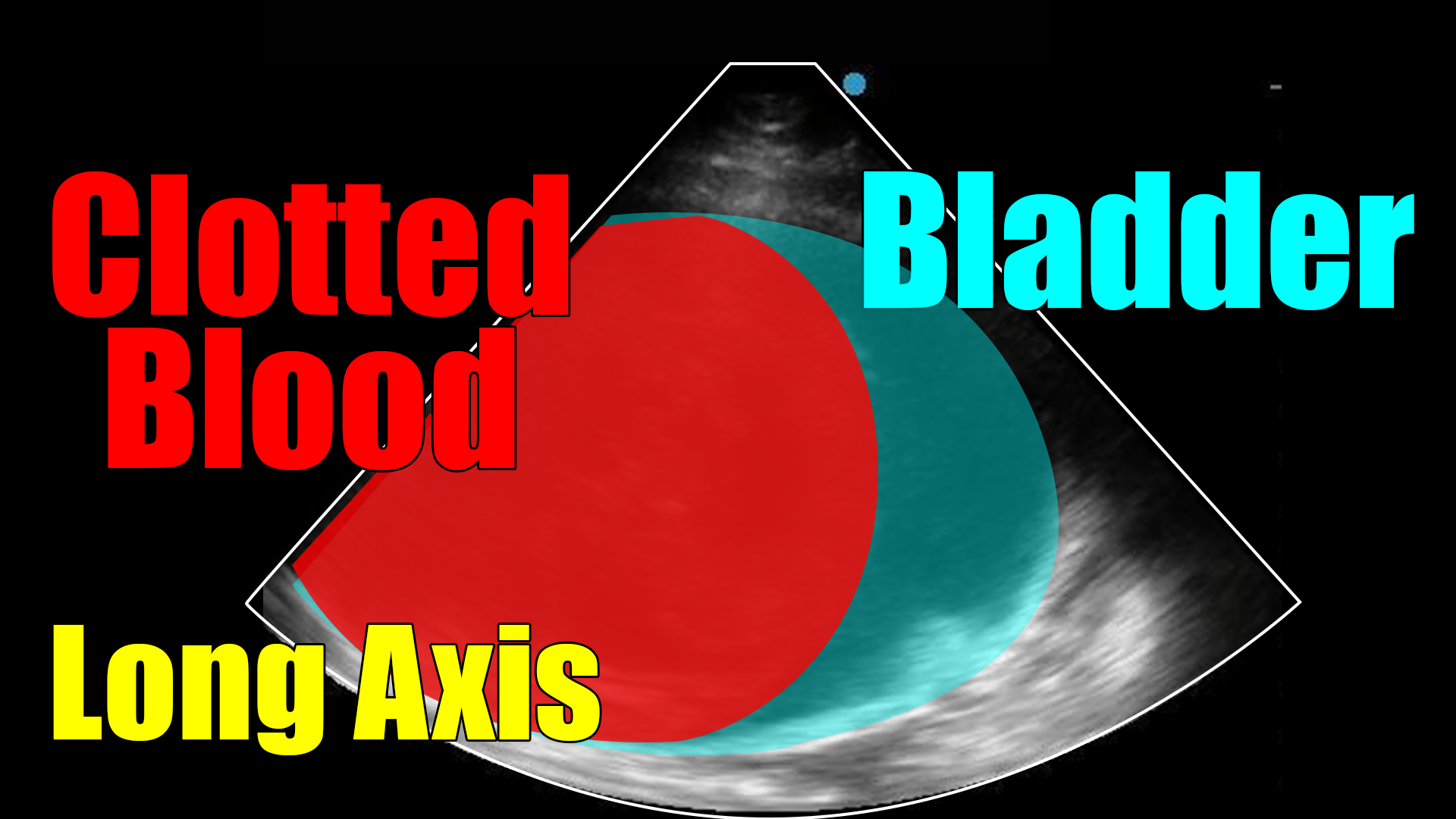
Unlike the prior case, what we see here is clotted blood. However, this case contains elements from both of the prior cases and illustrates the usefulness of the scan.
In terms of a catheter that returns blood (as was the case in the prior post) this scan showed us instantly that the issue was not malpositioning, but rather that the bladder was full of clots. In the first few seconds of the clip the balloon can be seen in the bladder.
In regards to the prior case in this post (case 2), this image illustrates what clotted blood looks like as compared to tumor. Notice in this case that the hematoma is rounded and the edge corresponds to the shape of the bladder wall. That suggests a gelatinous consistency (blood and clot) as opposed to a more solid mass (tumor), which does not form in the shape of the container (the bladder in this case).
Clearly having blood in the bladder does not rule out having a tumor, and the diagnosis is not complete based on these images. But it is a nice guide as to what the next steps should be.
In terms of management of case three, when we saw how much clotted blood was present, we decided on a trial of continuous bladder irrigation. Not surprisingly given the clot burden, that failed and she ultimately required cystoscopy for clot evacuation.
Let’s summarize what we’ve looked at so far. Cases one and three show us the utility of bladder ultrasound in the setting of a Foley catheter returning blood. Instantly the scan differentiates a bladder full of clot from a malpositioned catheter. Case two showed an instance where a presumed diagnosis of BPH was proven incorrect with a quick look at the bladder. All were small investments of our time that payed off in time to diagnosis.
