For the sake of argument, let’s say that a patient has a pulmonary embolism. Their blood pressure is low, and they are toxic appearing. They get tPA and an ICU admission. Let’s also say, purely hypothetically, that one of their admission diagnoses was cardiogenic shock. Perhaps that’s a simple oversight. Perhaps, however, there is a knowledge gap. If these theoretical doctors have some confusion about the categories/causes of shock, other might as well. Do you know what type shock is caused by a pulmonary embolism?

What is Shock?
UpToDate defines shock as a life-threatening condition of circulatory failure causing inadequate oxygen delivery to meet cellular metabolic needs and oxygen consumption requirements producing cellular and tissue hypoxia.
What causes Shock?
Oxygen delivery can be insufficient for reasons other than circulatory failure in a hydrostatic sense. Those include severe anemia or mitochondrial dysfunction due to carbon monoxide poisoning among others. Technically, those would cause “shock”. However, when considering causes of shock, we generally consider four circulatory conditions that impair delivery of oxygen to tissues, and that’s what will be described here.
In a big picture sense, perfusion can be compromised when the heart fails as a pump or when there is insufficient blood volume for tissue perfusion and maintenance of cardiac preload. The heart can fail due to intrinsic problems to the heart itself; or it can fail due to extrinsic mechanical forces. Blood volume can be low because of actual volume losses; or it can be low due to the loss of vascular tone such that the tank is acutely larger than it was at baseline. That’s really all there is to it, but let’s take a closer look.
Cardiogenic Shock
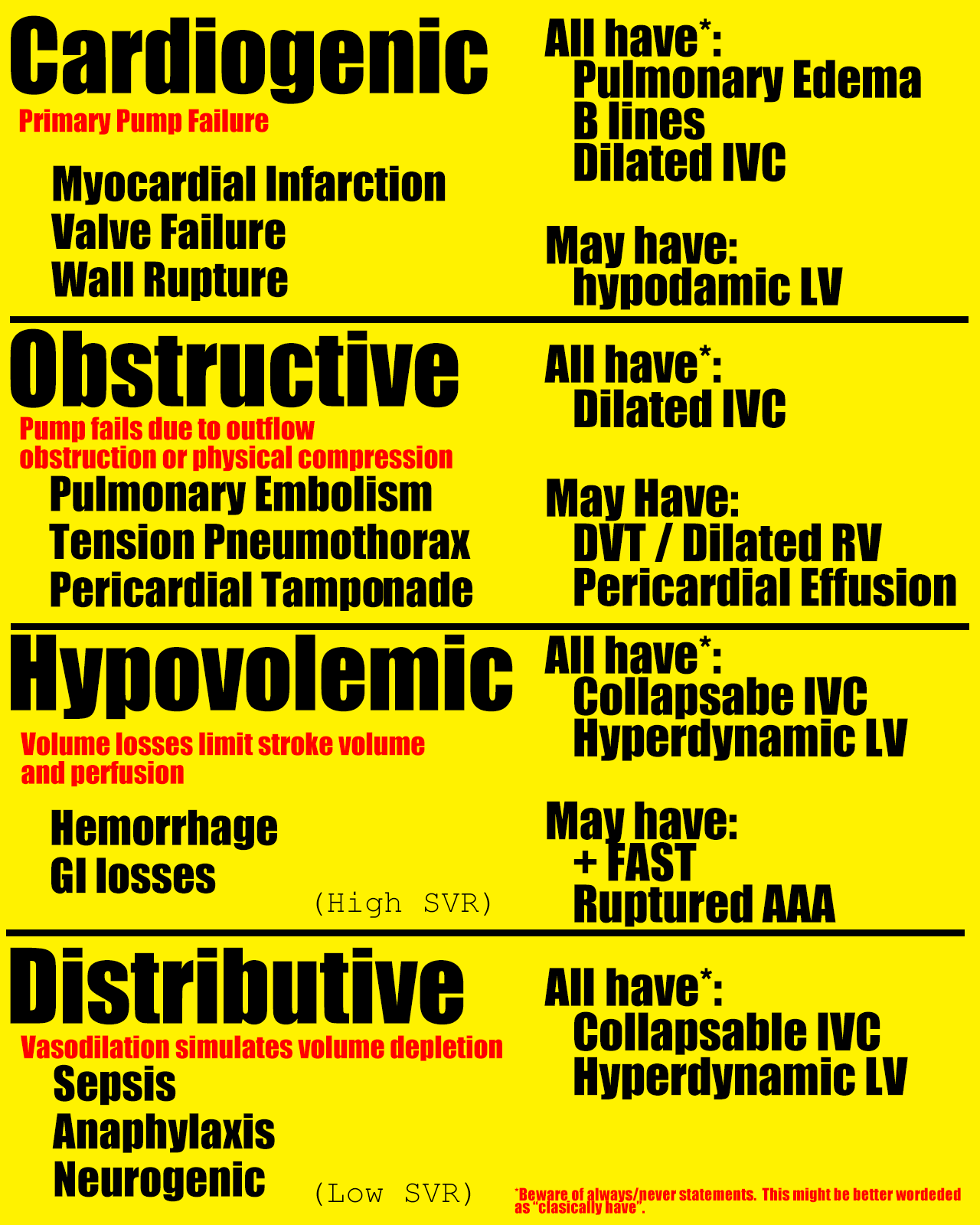
Cardiogenic shock occurs when circulation is inadequate due to primary failure of the heart as a pump. Causes include myocardial infarction and valve rupture. In terms of hemodynamic parameters, the cardiac output would be low, preload (pulmonary capillary wedge pressure) would be high, and systemic vascular resistance would be high. Clinically, these patients have pulmonary edema on exam. Ultrasound would show a dilated IVC. In the case of an MI, you would expect a hypodynamic left ventricle or wall motion abnormality.
Obstructive Shock
Obstructive shock occurs when the heart fails as a pump due to forces impeding flow that are outside the heart itself. Causes include strain from a pulmonary embolism or tension pneumothrax, or direct compression from pericardial tamponade. Although lumped together under this heading, pulmonary embolism and pericardial tamponade cause the heart to fail by very different mechanisms and there is no tidy way summarize their hemodynamic parameters that would fit all causes. You would universally expect a dilated IVC in these cases, however. These patients will show sings of right ventricle failure (dilated IVC) but may not show signs of left ventricle failure (pulmonary edema) as the obstruction is often upstream from the left ventricle, i.e. in the lungs. In the setting of embolism, cardiac ultrasound would show a dilated right ventricle and a DVT might be found on exam of the lower extremities. Pericardial effusion would be noted in the case of tamponade.
Hypovolemic Shock
Hypovolemic shock occurs when plasma volume is lost due to hemorrhage, vomiting, diarrhea, or insensible losses (heat exposure, for example). Cardiac output is low; SVR is high. This is usually easy to recognize based on history. Exam might show a positive FAST exam or AAA. Cardiac exam will show a hyperdynamic left ventricle with a compressible or even flat IVC.
Distributive Shock
Distributive shock occurs due to loss of vascular tone. The most common cause is sepsis. In terms of hemodynamic profile, distributive shock is differentiated from hypovolemic shock by having a low SVR. That being said, SVR is not a measurement we generally consider in the ED. Thankfully, these two are usually easily sorted based on history (vomiting, hemorrhage, or heat exposure suggests hypovolemic shock) and exam (fever, identifiable infection, and luekocytosis favor distributive shock). Luckily, fluids are treatment for both, though vasopressors may be necessary in distributive shock states. Cardiac exam will usually show a hyperdynamic left ventricle and collapsible IVC as was the case for hypovolemic shock.
What about our case?
Pulmonary emboli cause obstructive shock. The pump would work fine if it weren’t for the blood clot obstructing the outflow from the right ventricle.

Great read, Dr. Steele! I did have one question – you mention that preload is similar to the pulmonary cap wedge pressure (PCWP). I always thought that PCWP was an estimate of LAP and LVEDV (preload of the LV)? PCWP won’t tell us what the preload of the RV is though, correct? Hope I’m understanding that correctly.
LikeLike
You have it right. When we talk about preload of the heart as a whole, we are generally referring of the left ventricle. The pulmonary capillary wedge pressure is a surrogate for left ventricle preload. Right sided pressures can be measured directly or a CVP can be used as an estimate.
An elevated CVP in isolation does not tell us the cause of the elevated pressure on the right side. It could be due to elevated left sided pressures or isolated right sided failure. Usually we can sort that out with history and exam.
LikeLike