
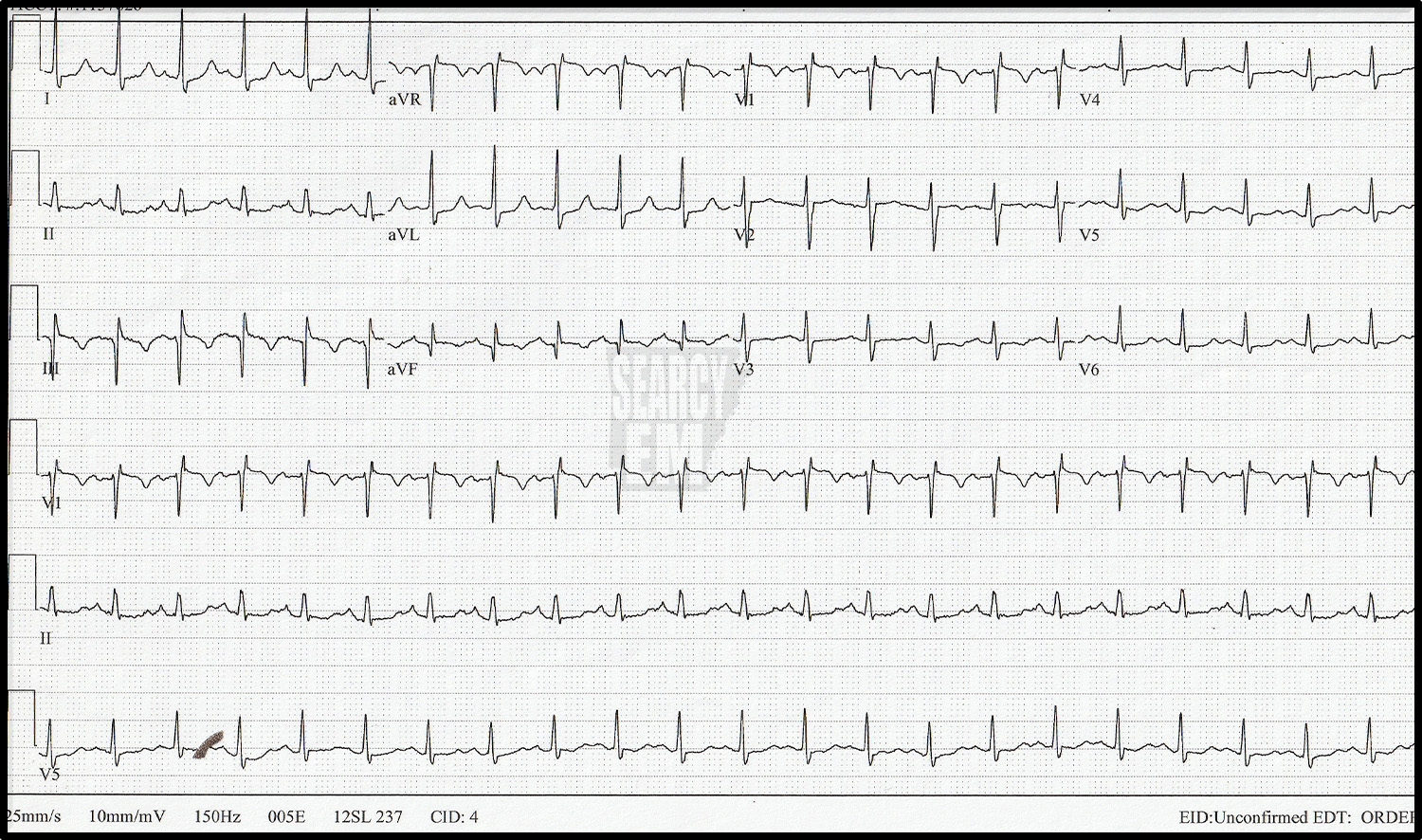
69 Interpretation
Narrow, regular, and extremeley fast at 258 bpm. This most likely SVT. With a rate that fast I’d wonder if there was a bypass tract. could this be afib in the setting of WPW and it is going so fast that I don’t apprecaiate its irregularity? Perhaps, but it is most likely SVT.
24 Interpretation
Wenchebach, Second degree AV block type 1, (Mobitz 1)
38 Interpretation
Mobitz 2 second degree AV block
Probably a third degree AV block. It appears that the P waves are coming at the same rate as the QRS complexes, though. Could this be a sinus rhythm with a huge primary AV block? I don’t we can say for certain that it can’t be that. This is the same patient as in 38a and the QRS complexes here look exactly like the sinus QRS complexes from the 38a, which raises the possibitliy that we are seeing sinus conducted QRS complexes here (i.e. a primary AV block). The other possibility is that none of the P waves are being conducted and every other one is buried in the QRS complex and that the QRS rate just happens to be exactly half of the P wave rate. That would make this Third degree block. We would need to see a longer strip to look for some irregularity to know for sure.
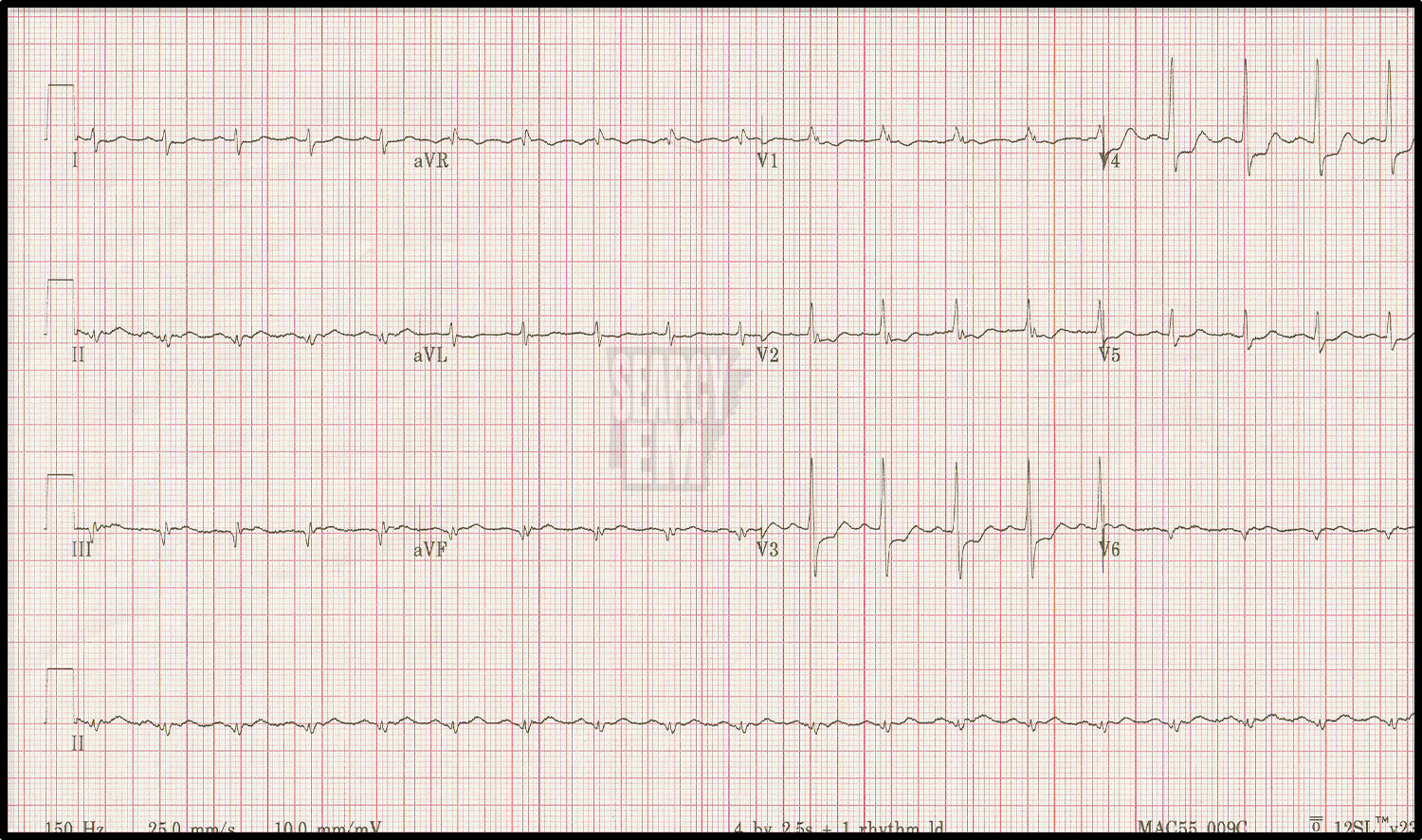
13 Interpretation
Sinus, LAD, poor R wave progression
12 Interpretation
RBBB

72 Interpretation
Brugada pattern type 1
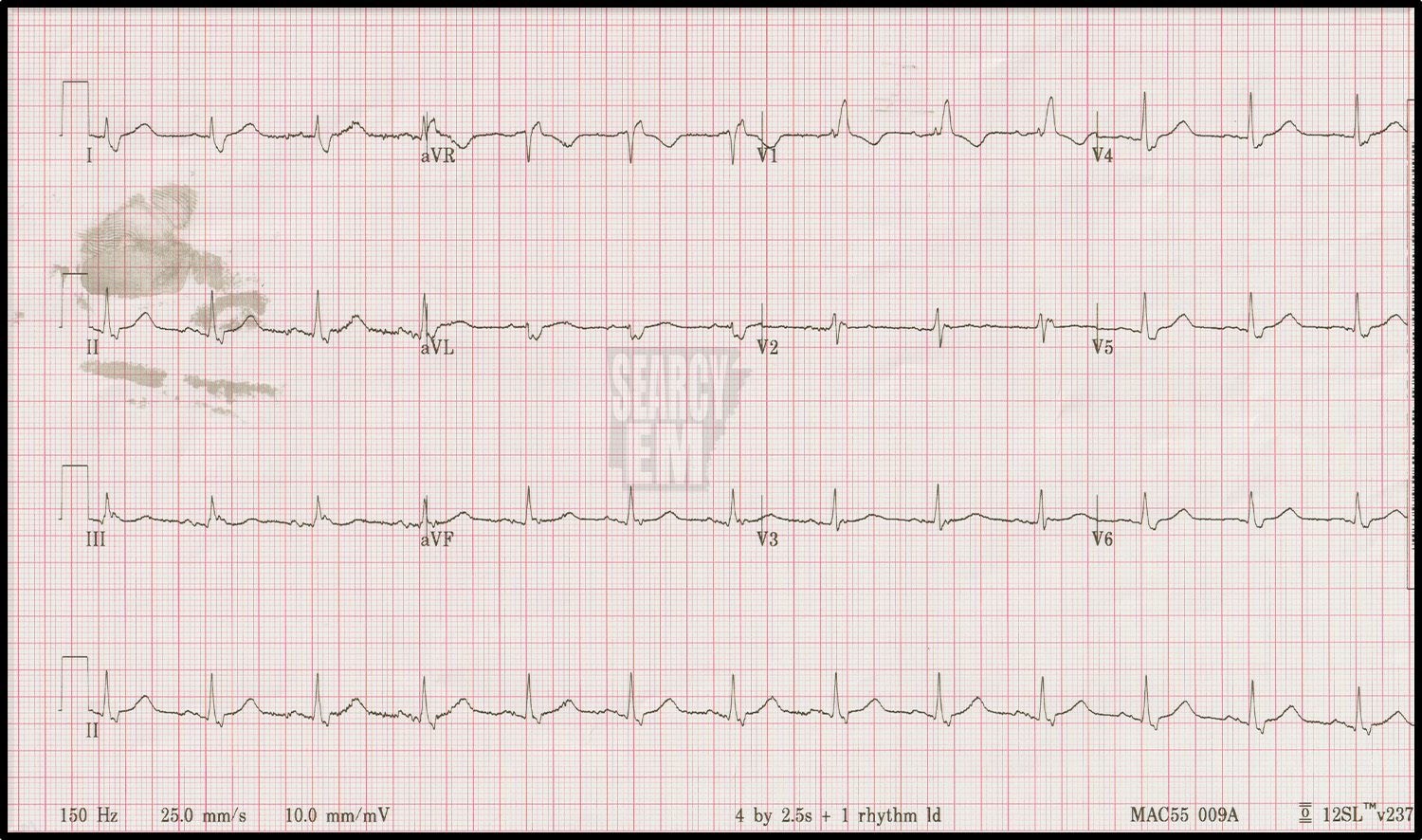
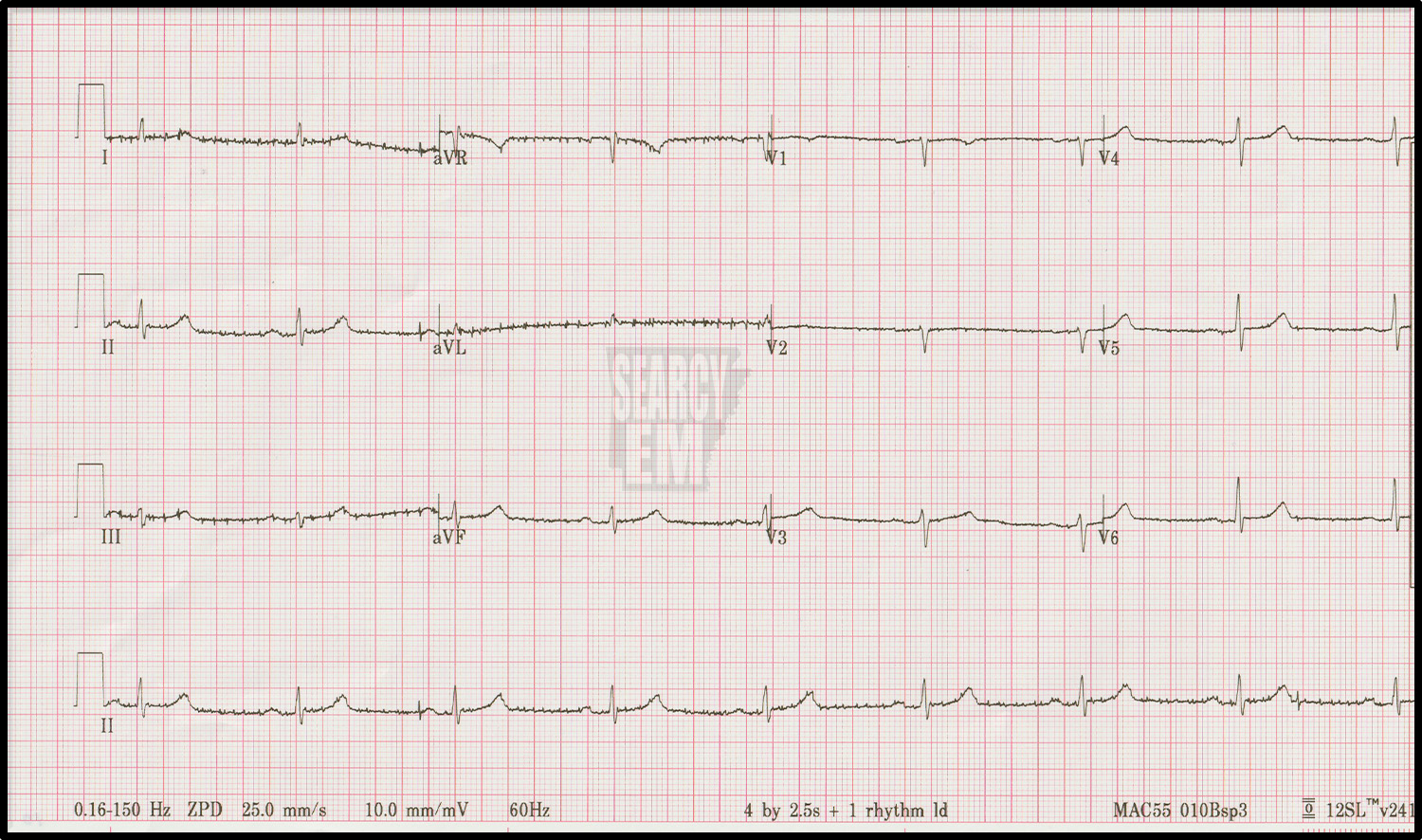
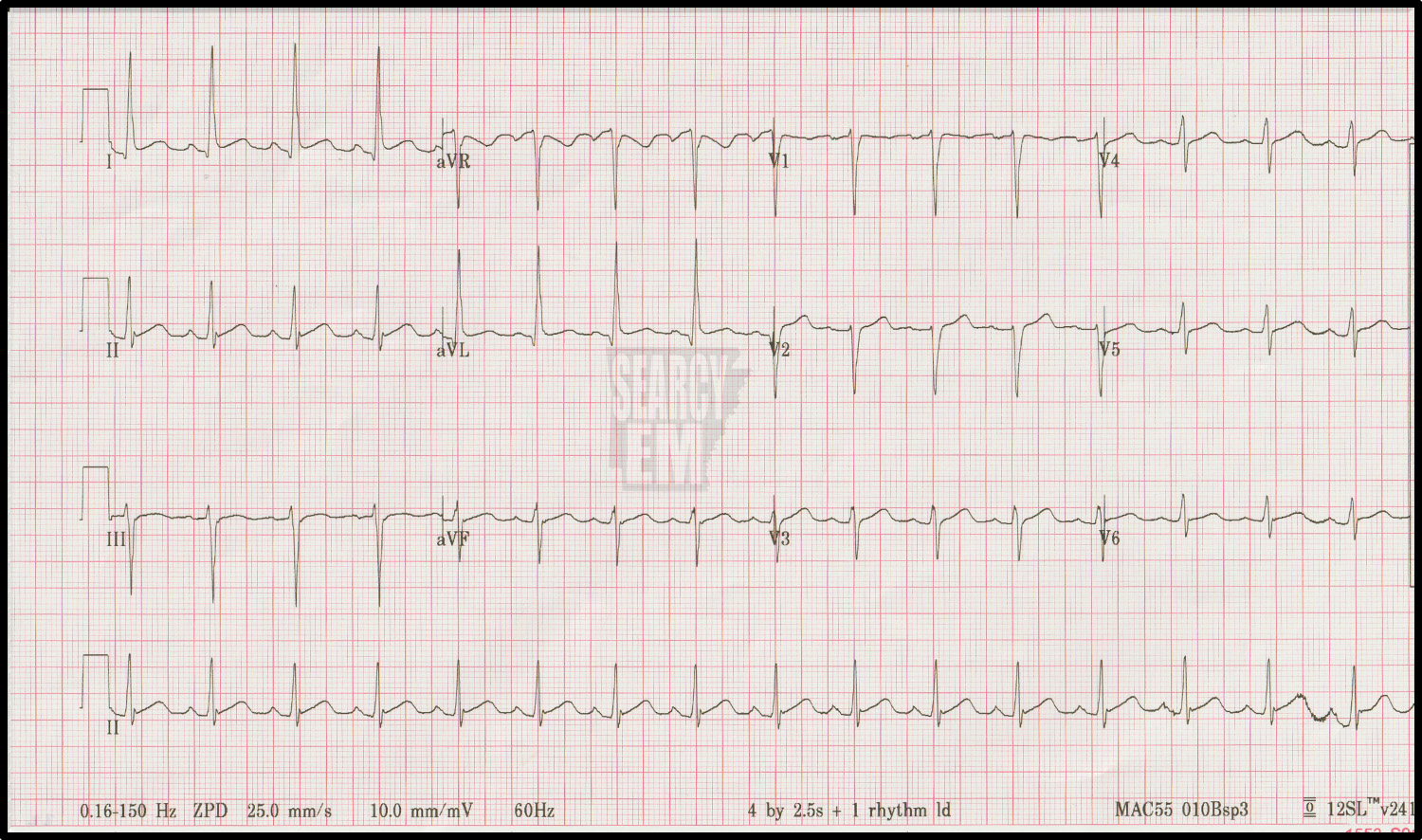
40 Interpretation
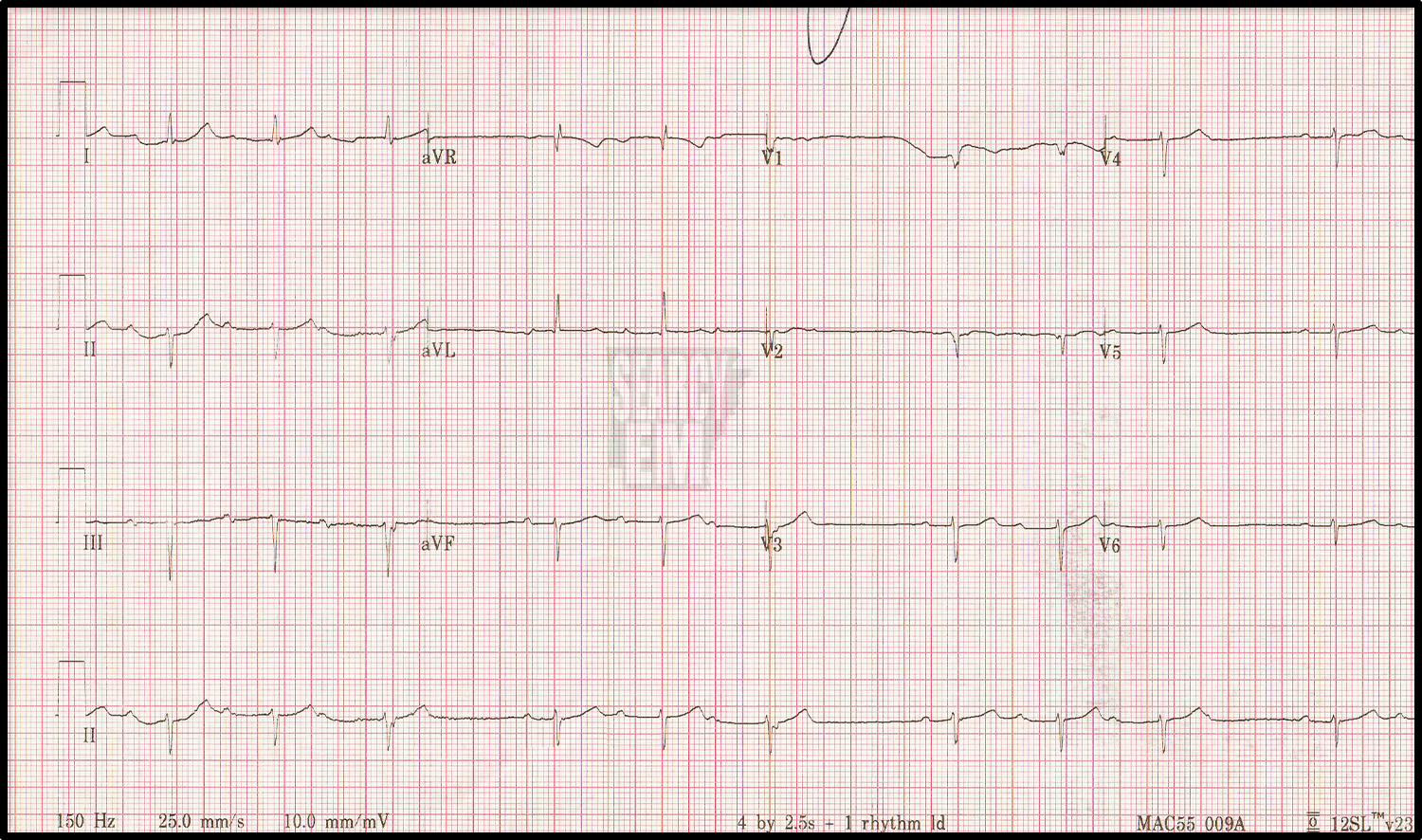
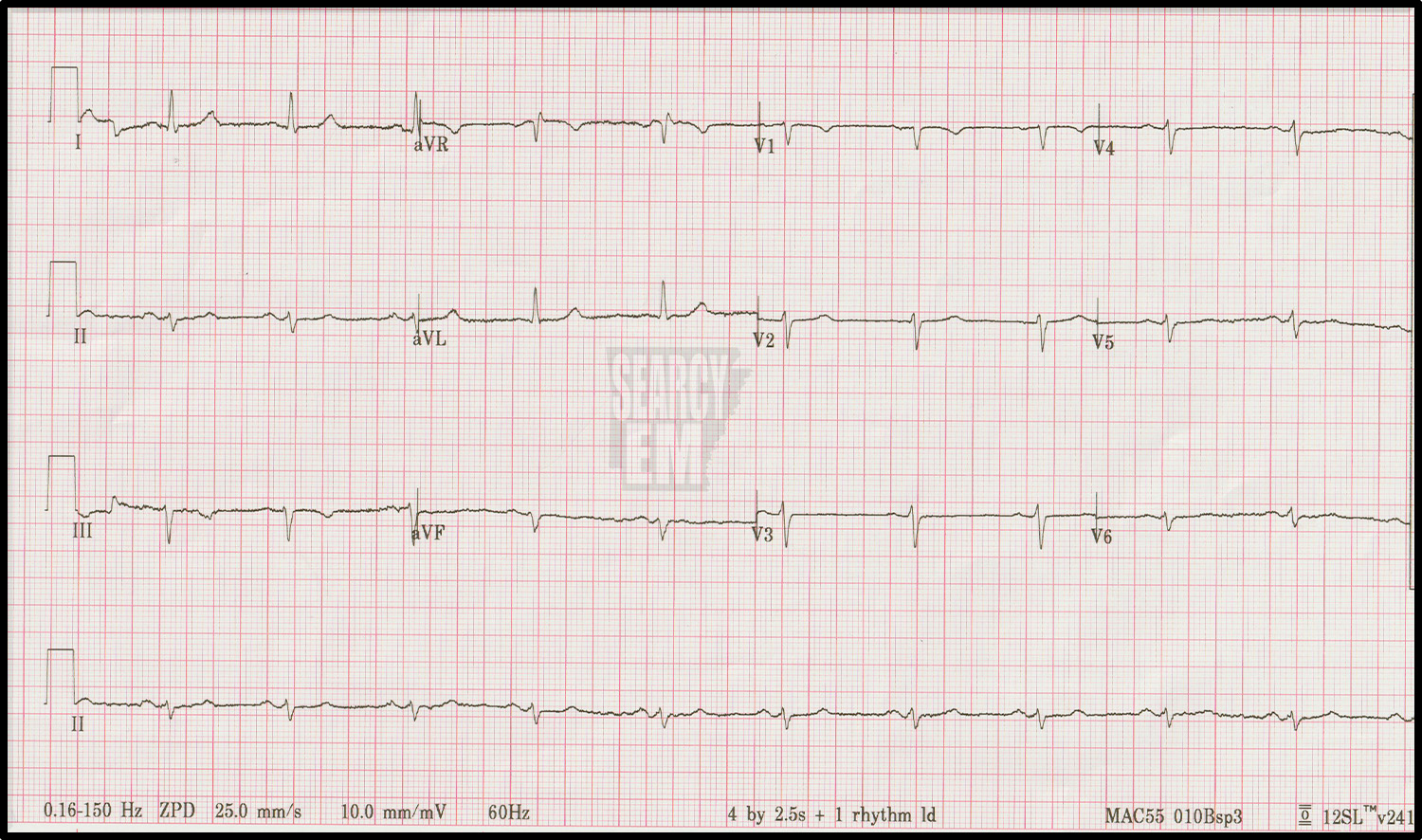
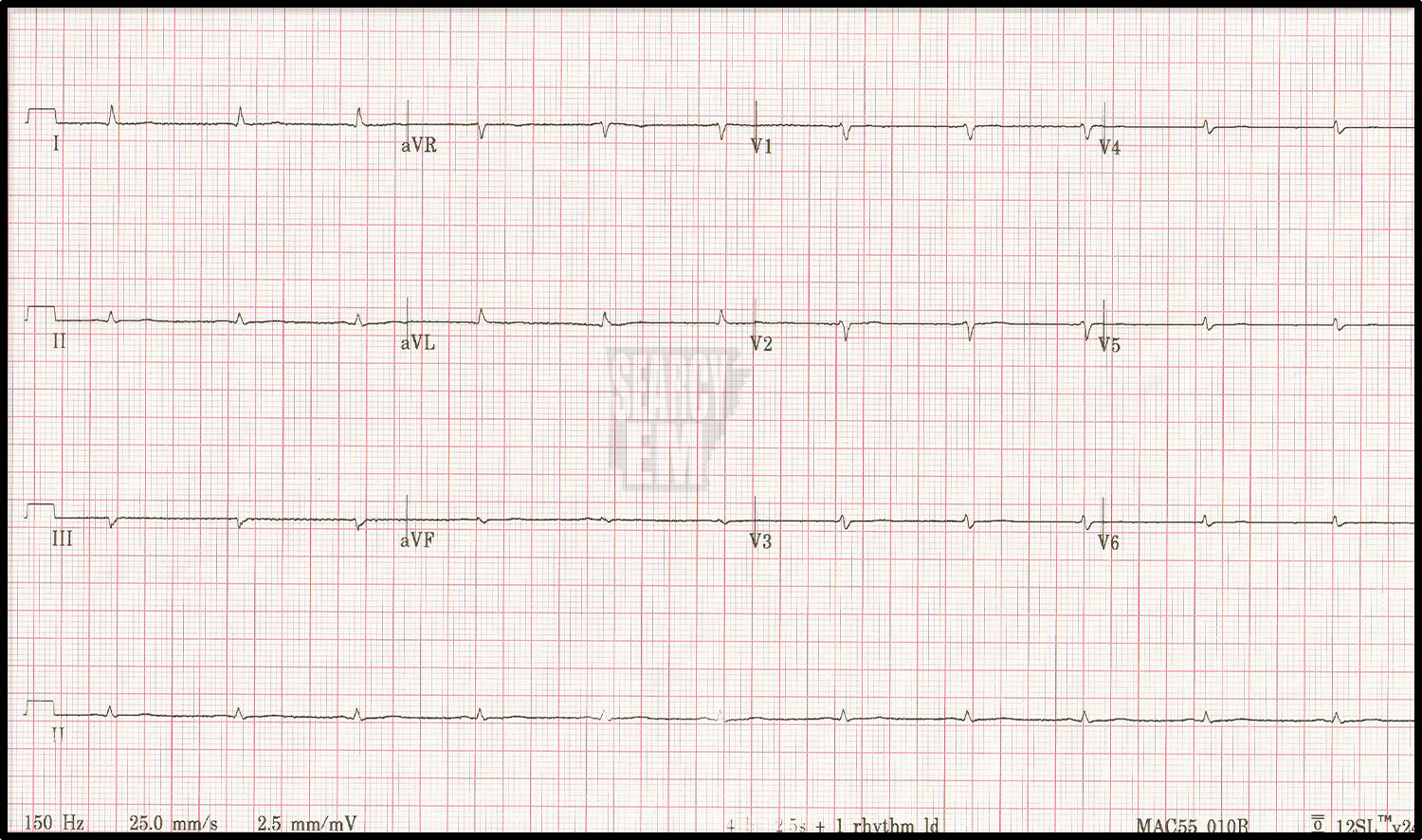
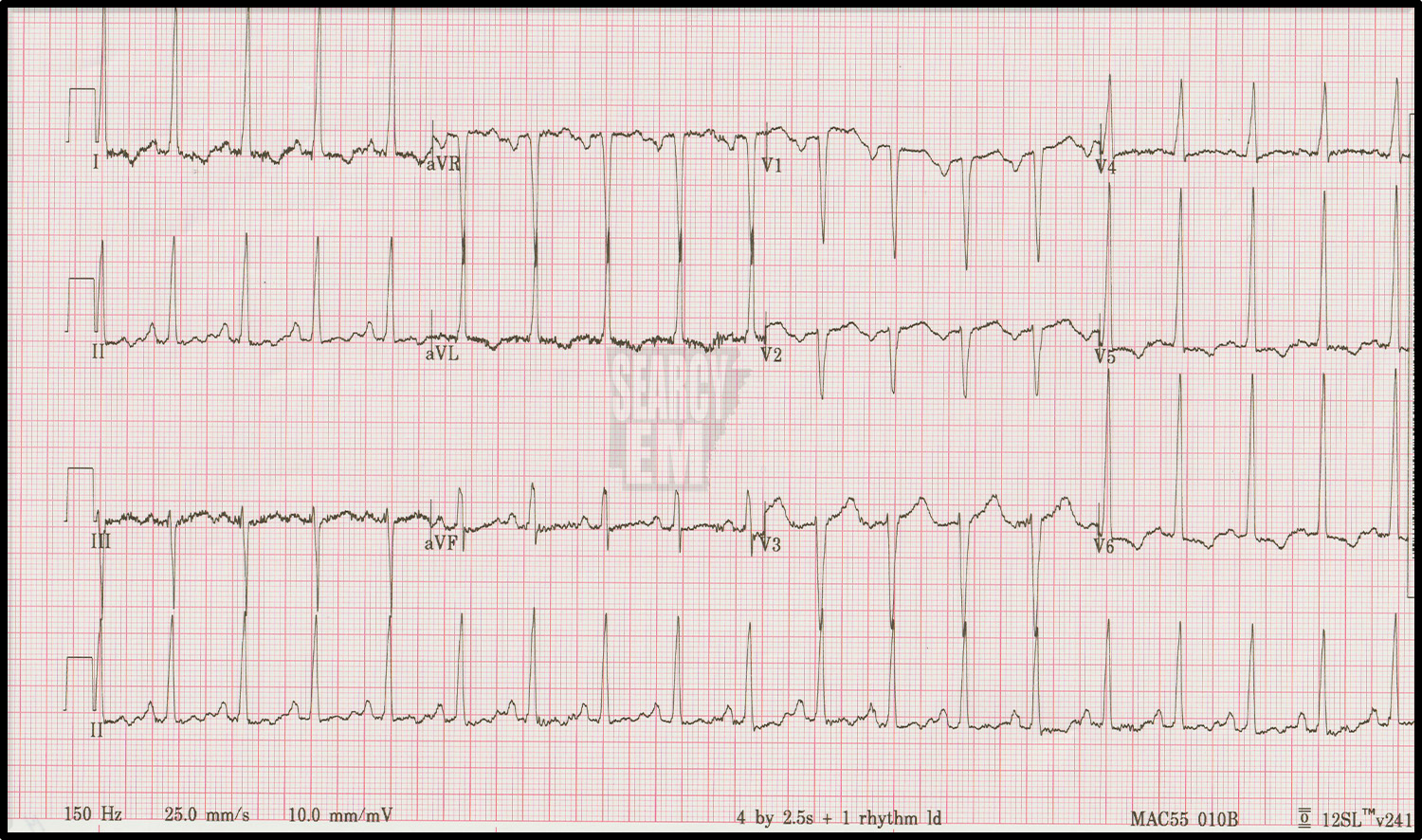
low voltage, sensitivity set to an odd setting: 2.5 mm/mV instead the typical 10mm/mV

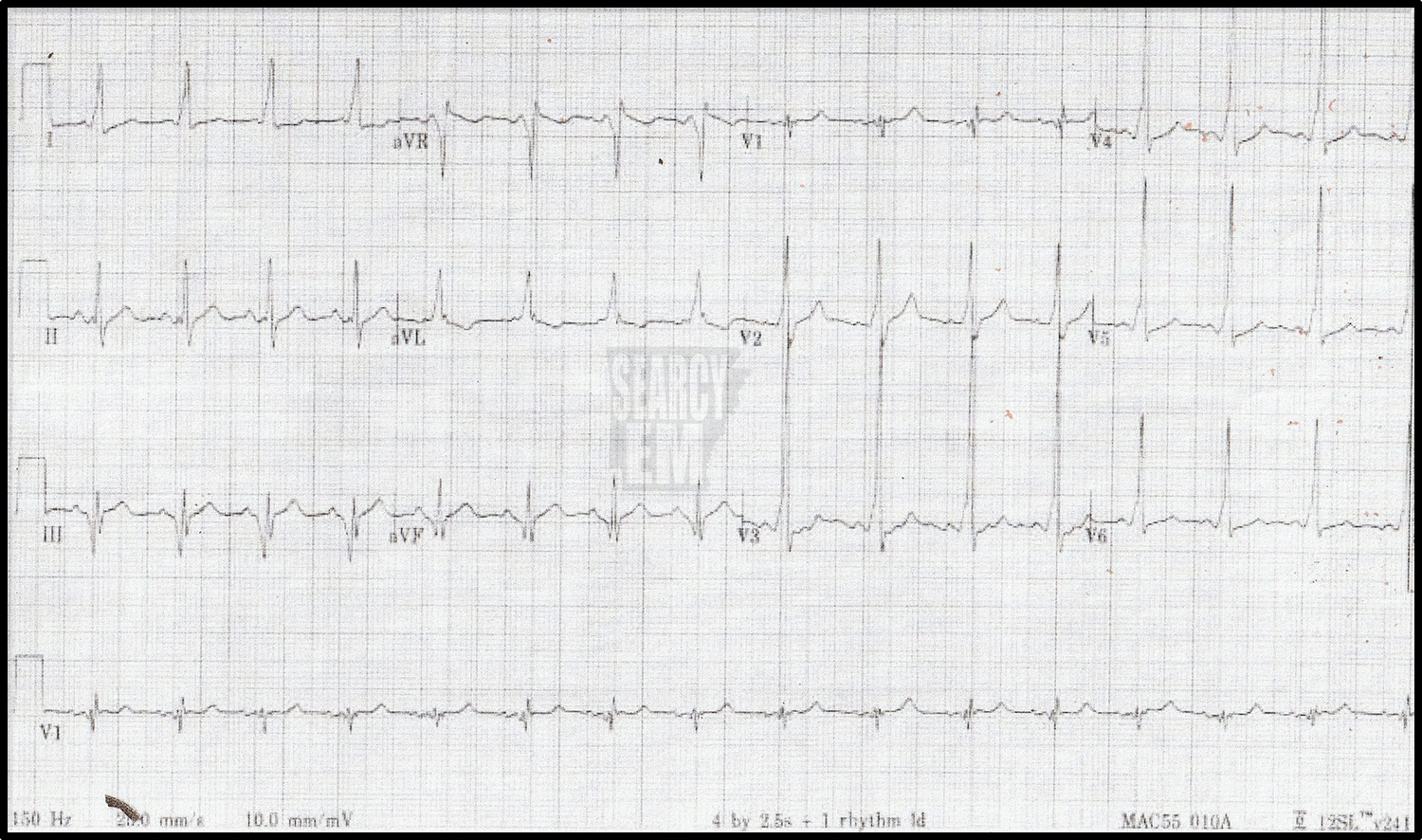
Same person/same time as EKG 40. The calibration has been corrected. This is a normal ekg.
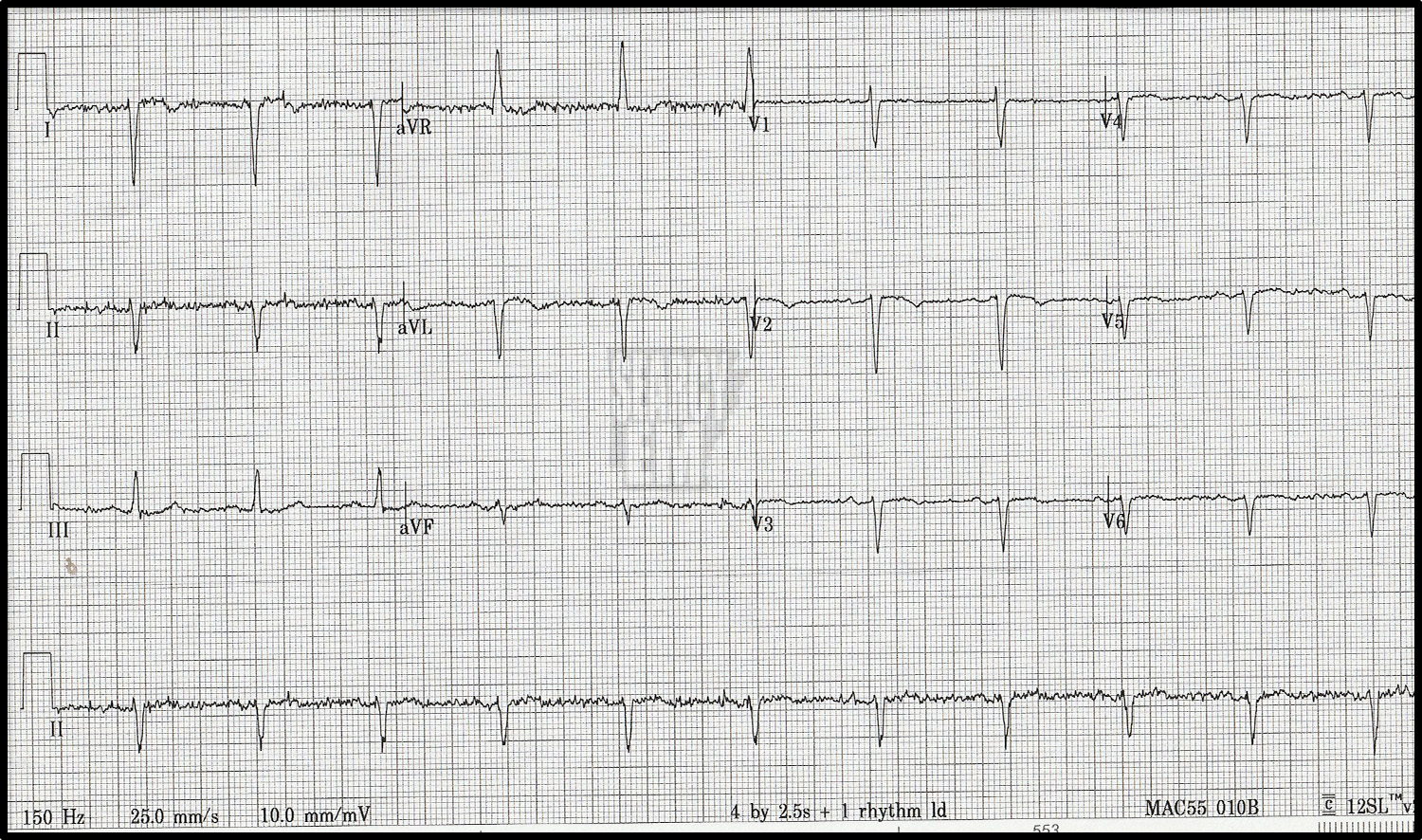
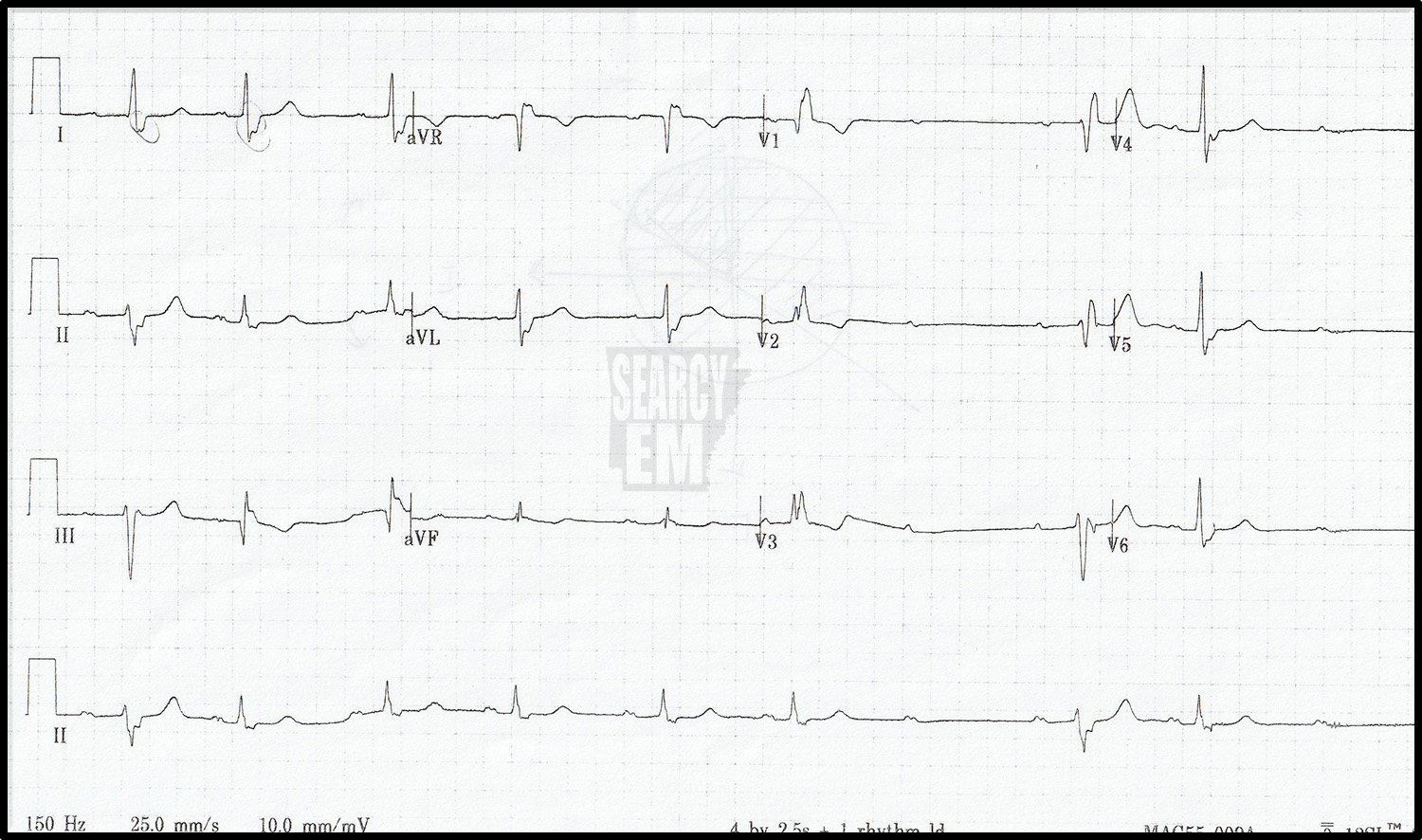
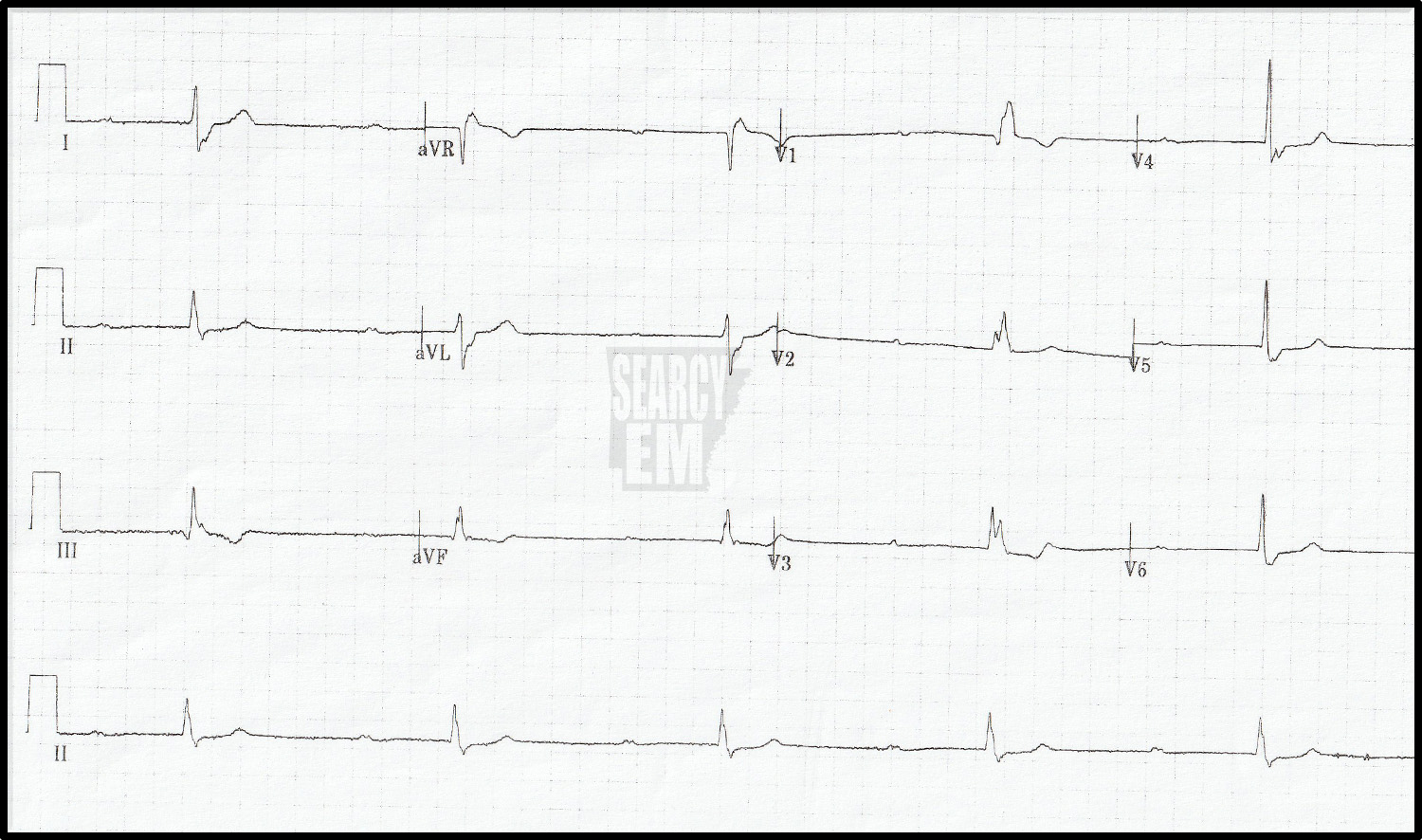
65 Interpretation
Down in I, up in aVR, concerning for limb lead misplacement. However, there are no R waves in the chest leads (other than V1, which is on the right side of the sternum). This is dextrocardia.
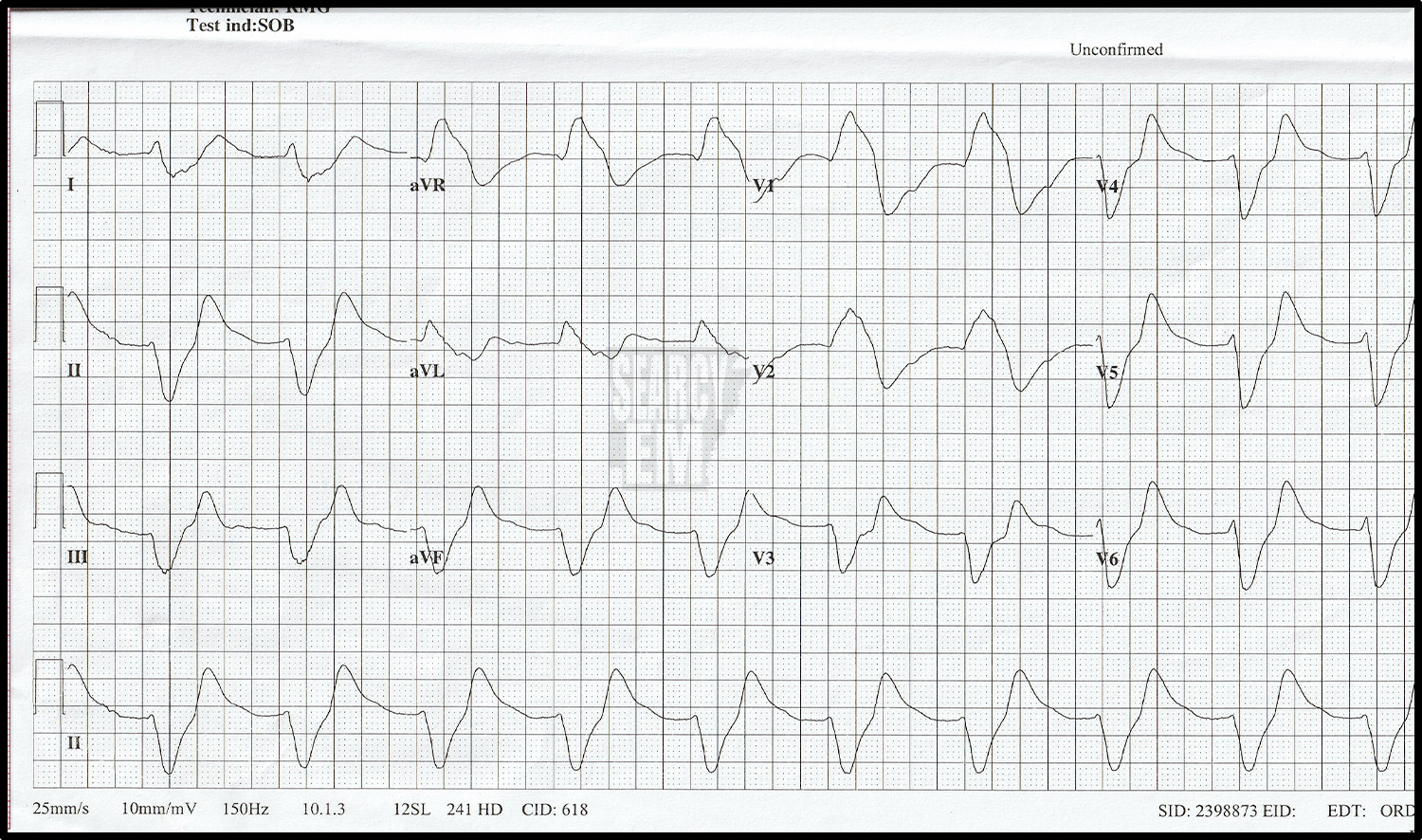
33 interpretation
Extremely wide QRS, no P waves. Hyperkalemia. Slow VT, and 3rd degree block are considerations, but this was hyperkalemia.

7 Interpretation
Normal
10 Interpretation
Normal

18 Interpreation
Sinus tachycardia. Notched QRS complexes in the inferior leads (frankly, I don’t know the significance of that finding). Otherwise normal
22 Interpretation
normal sinus, trace of elevation in v1 an aVL. Not diagnostic of STEMI. It catches my eye that the QRS is so negative in lead III and so positive in II. I’d have been interested to see what the machine read the R wave axis as.
61 Interpretation
Sinus tachycardia with S1Q3T3. This patient had a pulmonary embolism.
35 Interpretation
Sinus tachycardia with ST depression in V2-V4. Concerning for anterior ischemia vs posterior infarction.

The same patient as EKG 35. In this tracing, leads V4, V5, and V6 have been moved to positions V7, V8, and V9. The depression remains in the anterior leads (V2, V3), but now we see ST elevation in leads V7-V9). This is a posterior STEMI. You can see that the leads 7, 8, and 9 were hand written in on the tracing as the machine does not know that the leads were moved.
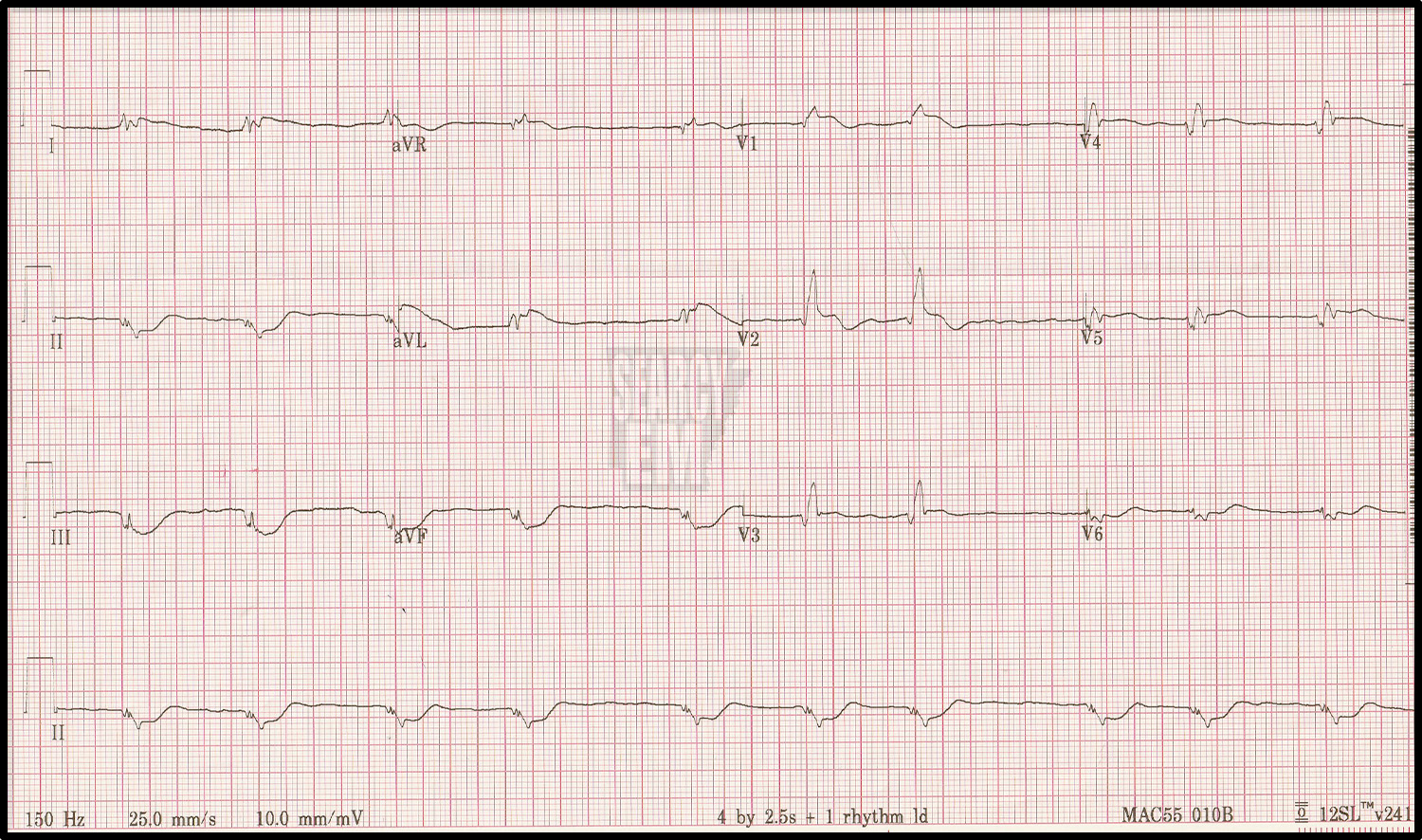
48 Interpretation
Sinus rhythm with ST elevation in the inferior and lateral leads: Inferiolateral STEMI.

57 Interpretation
Sinus with ST depression in the anterior leads. Concerning for anterior ischemia vs posterior infarction.
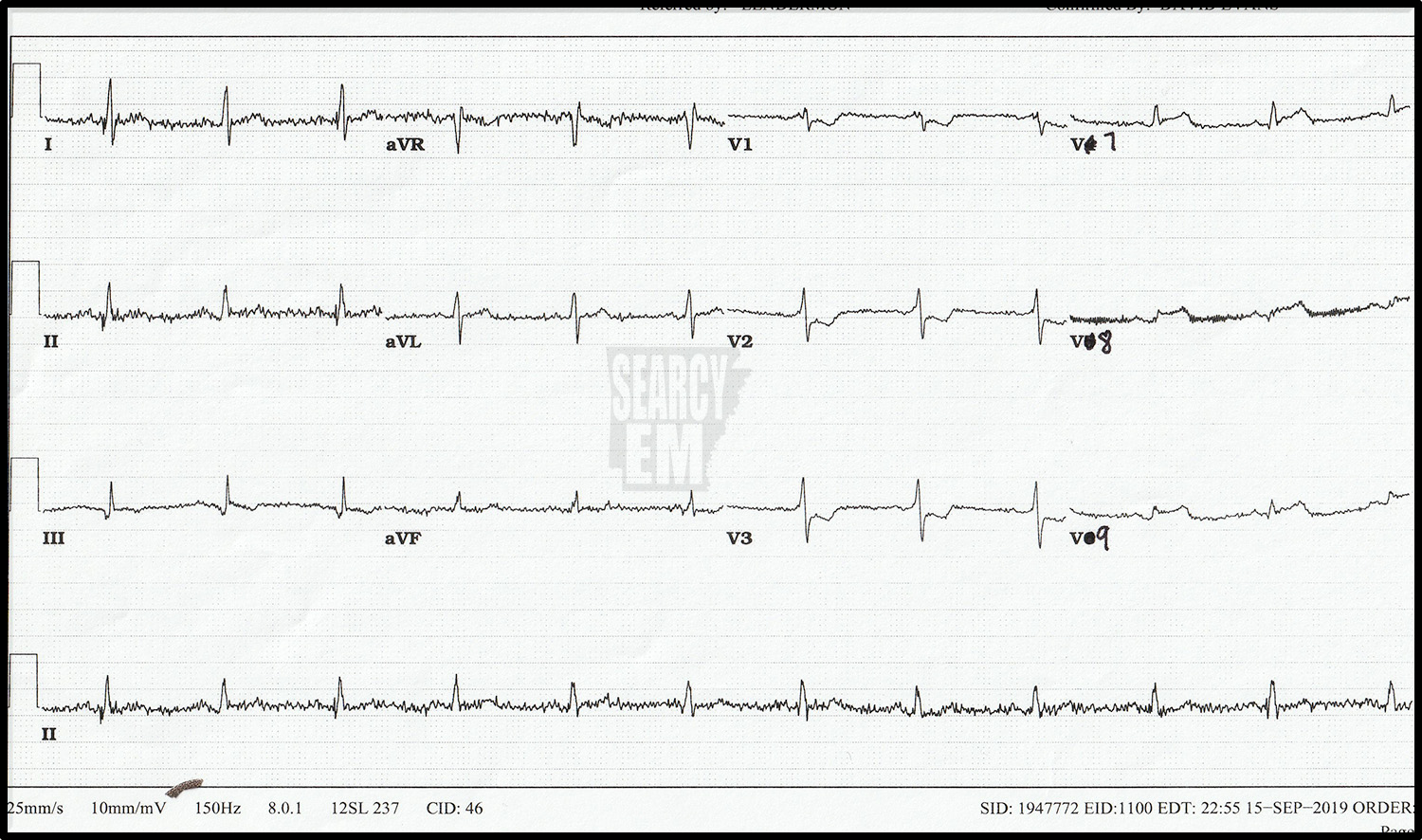
The same patient as EKG 57. In this tracing, leads V4, V5, and V6 have been moved to positions V7, V8, and V9. The depression remains in the anterior leads (V2, V3), but now we see ST elevation in leads V7-V9). This is a posterior STEMI. You can see that the leads 7, 8, and 9 were hand written in on the tracing as the machine does not know that the leads were moved.
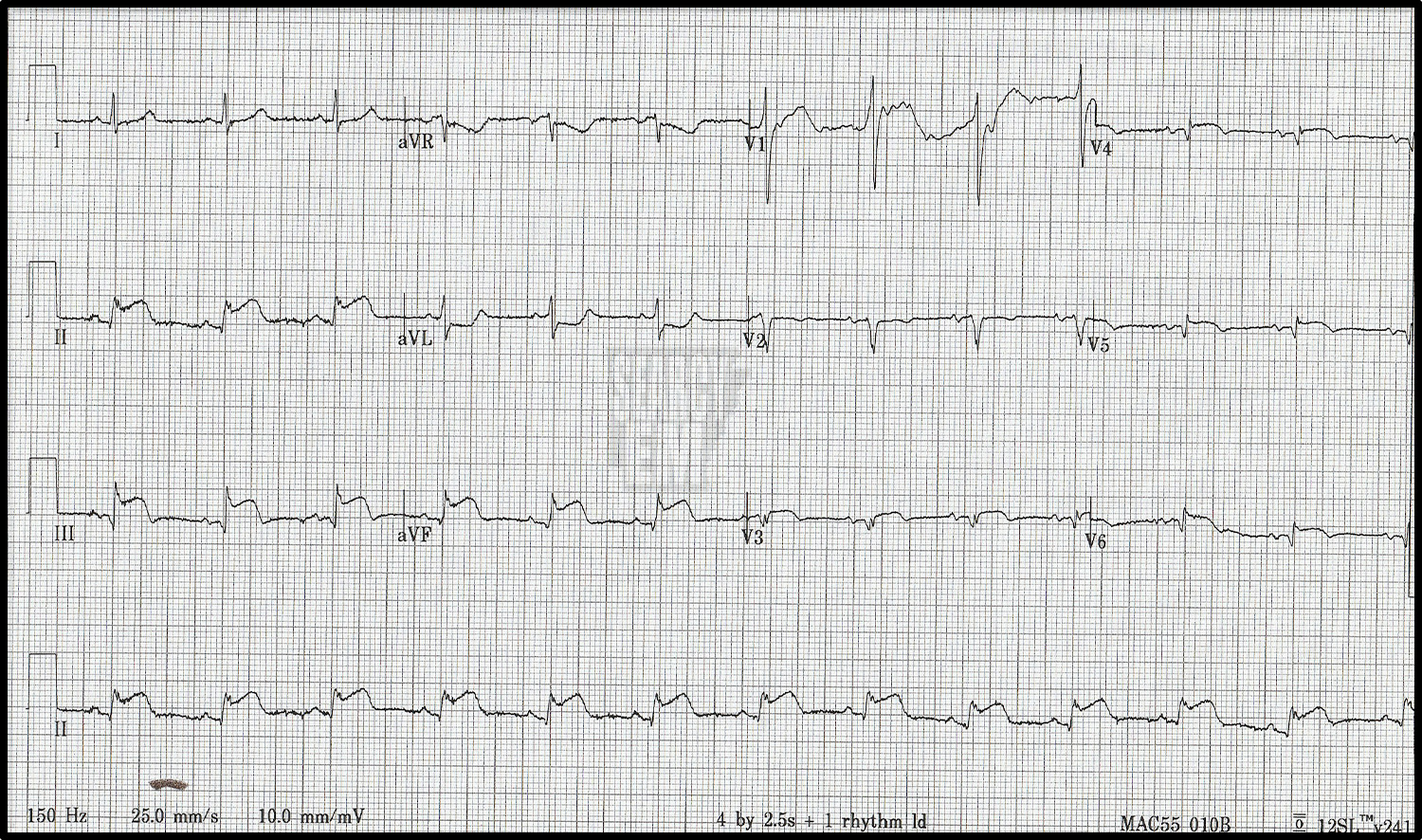
67 Interpretation
ST elevation in leads V1-V4 with ST depression in leads II, III, and aVF. Anterior STEMI.
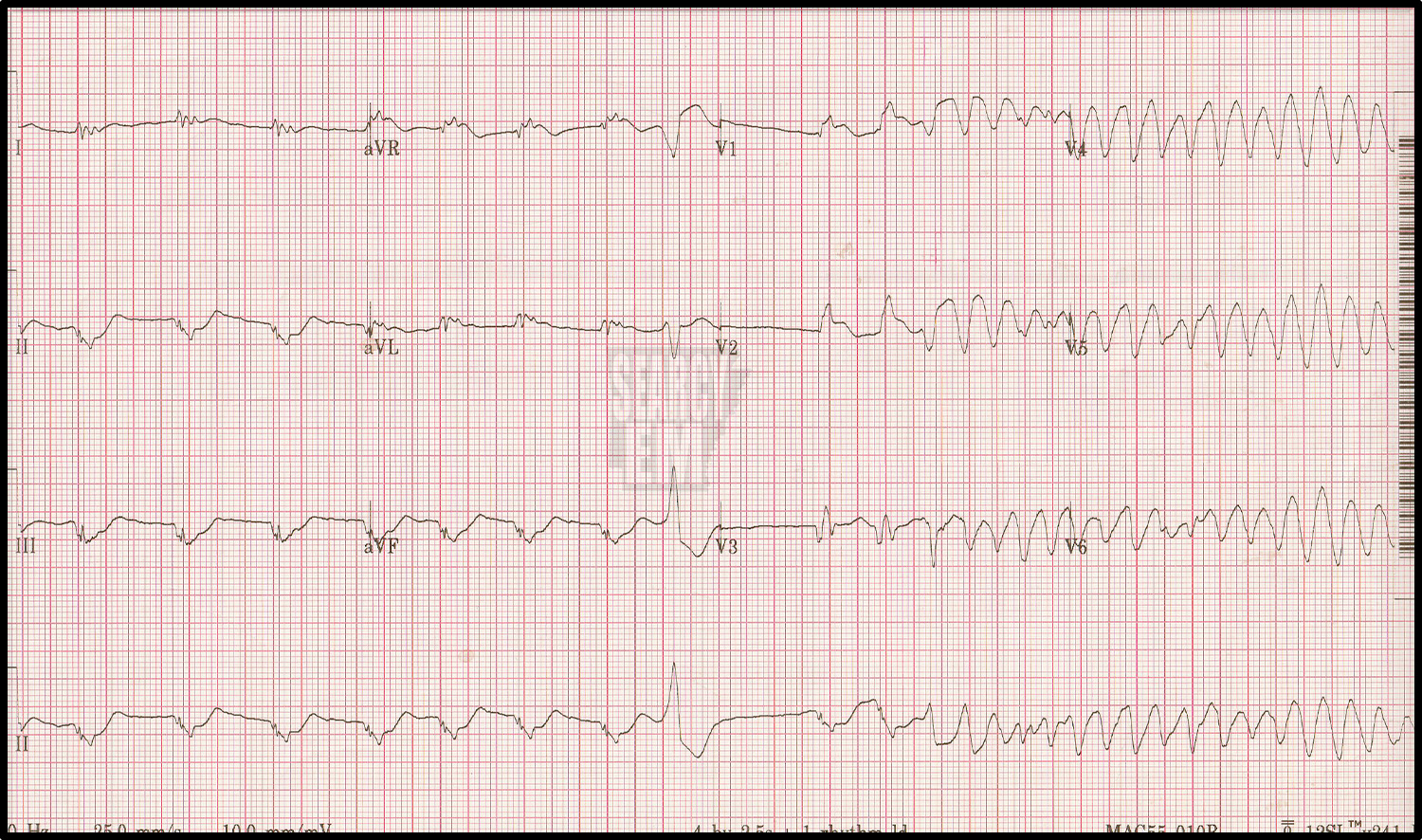
Same patient as EKG 67. in this tracing, we happen to catch them going into VT. It looks like polymorphic VT in this short segment, but in a longer stretch is may ‘settle’ into monomorphic VT.
14 Interpretation
Sinus Tachycardia. large voltages. TWI laterally.
53 Interpretation
WPW
