I’ve written posts before about times that the cardiac monitor disagrees with the pulse oximeter as to how many times the heart is beating. In the prior post, it was due to PVC’s. This time it is something different…

The cardiac monitor senses the electrical activity of the heart, while the pulse oximeter measures for pulsatile flow in the periphery – usually on a finger. Sometimes these things disagree, and we have to figure out which one is correct.
We see this frequently in the setting of bigeminy. I’ve also seen in hyperkalemia where peaked T waves are interpreted as QRS complexes by the cardiac monitor. I don’t recall ever having seen this, though.

In this case the P waves were so big that the cardiac monitor was mistakenly counting them as QRS complexes.
We obtained an ECG:
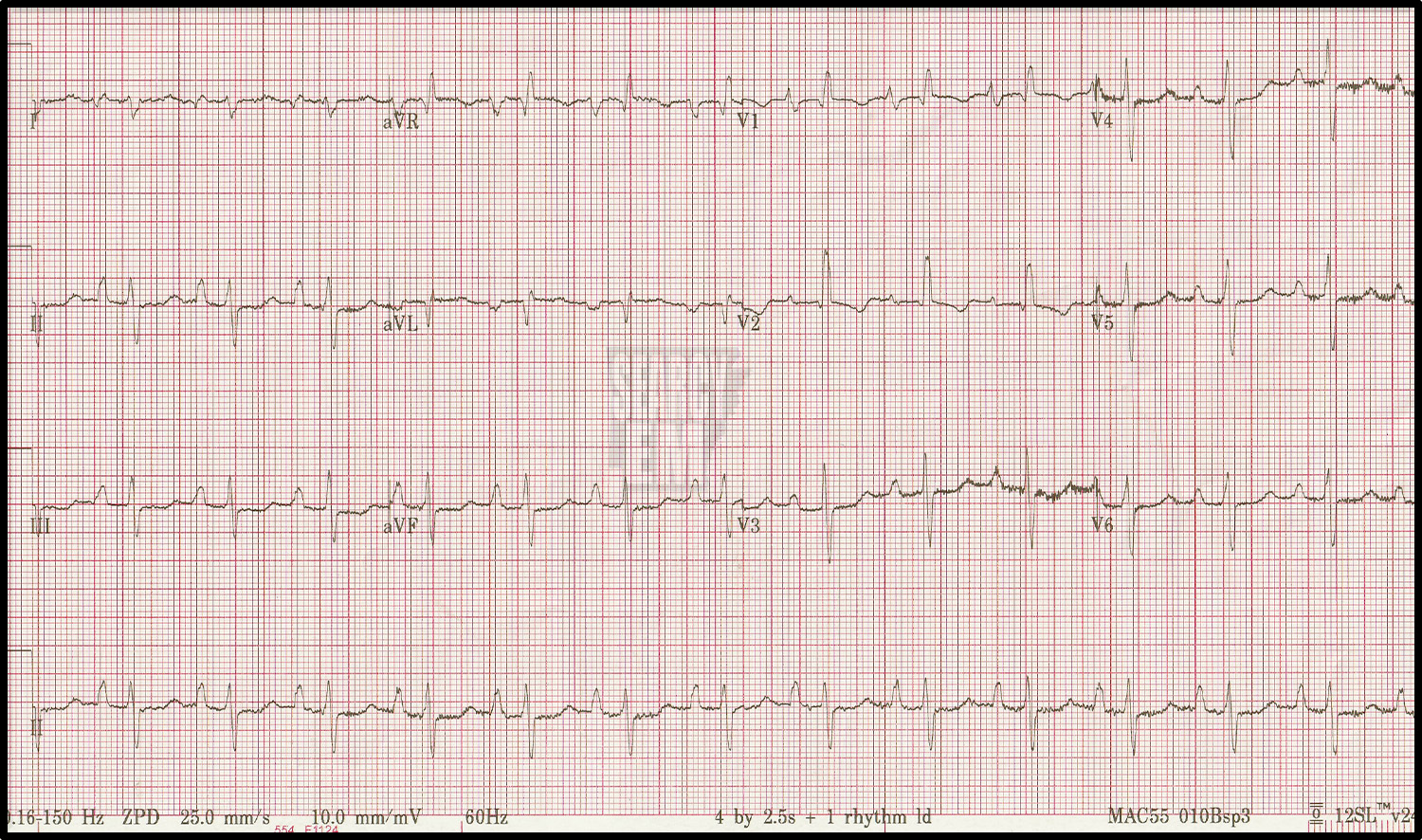
It shows sinus rhythm at rate of 78 bets per minute, extreme axis deviation (Northwest axis), no acute ischemic changes, poor R wave progression, but it is most noteworthy for the very tall P waves (at least 4 mm) in lead II. (Recall that normal is less than 2.5 mm.) This is called P pulmonale and is caused by right sided heart disease (pulmonary hypertension, COPD, tricuspid steonsis, etc.)
The patient did in fact have known, severe pulmonary hypertension.
I suspected they would have an impressive echo, which they did:
The right ventricle and atrium are dilated enormously. There is marked septal bowing. The IVC is plump and not collapsible.
This patient has pulmonary hypertension with all the fixings.
Wrap it up…
Chronic high pressures in the lungs (pulmonary hypertension) causes the right side of the heart to work harder than usual. Chronic hard work by the right side leads to right sided hypertrophy. Right ventricular hypertrophy can cause right axis deviation on the ECG (this patient has “extreme” axis deviation). Right atrial hypertrophy can be seen on the ECG as tall P waves in lead II (>2.5 mm), a finding called “P pulmonale”. These were so tall that they confused the cardiac monitor.
This case was a great example of some of the pathology caused by pulmonary hypertension.
