A 68 year-old man was sent by his PCP for evaluation of abnormal outpatient labs. He had been seen last week for back pain and malaise. We had a look at the labs and the diagnosis was there. Do you see it? What should the next test be?
This might be the least emergency medicine post I’ve ever made. However, this is based on a case that I saw with the residents where it was clear that not everyone on the team understood all the inner workings of the pathology. So, I’ll take the opportunity to tighten some of our internal medicine screws.
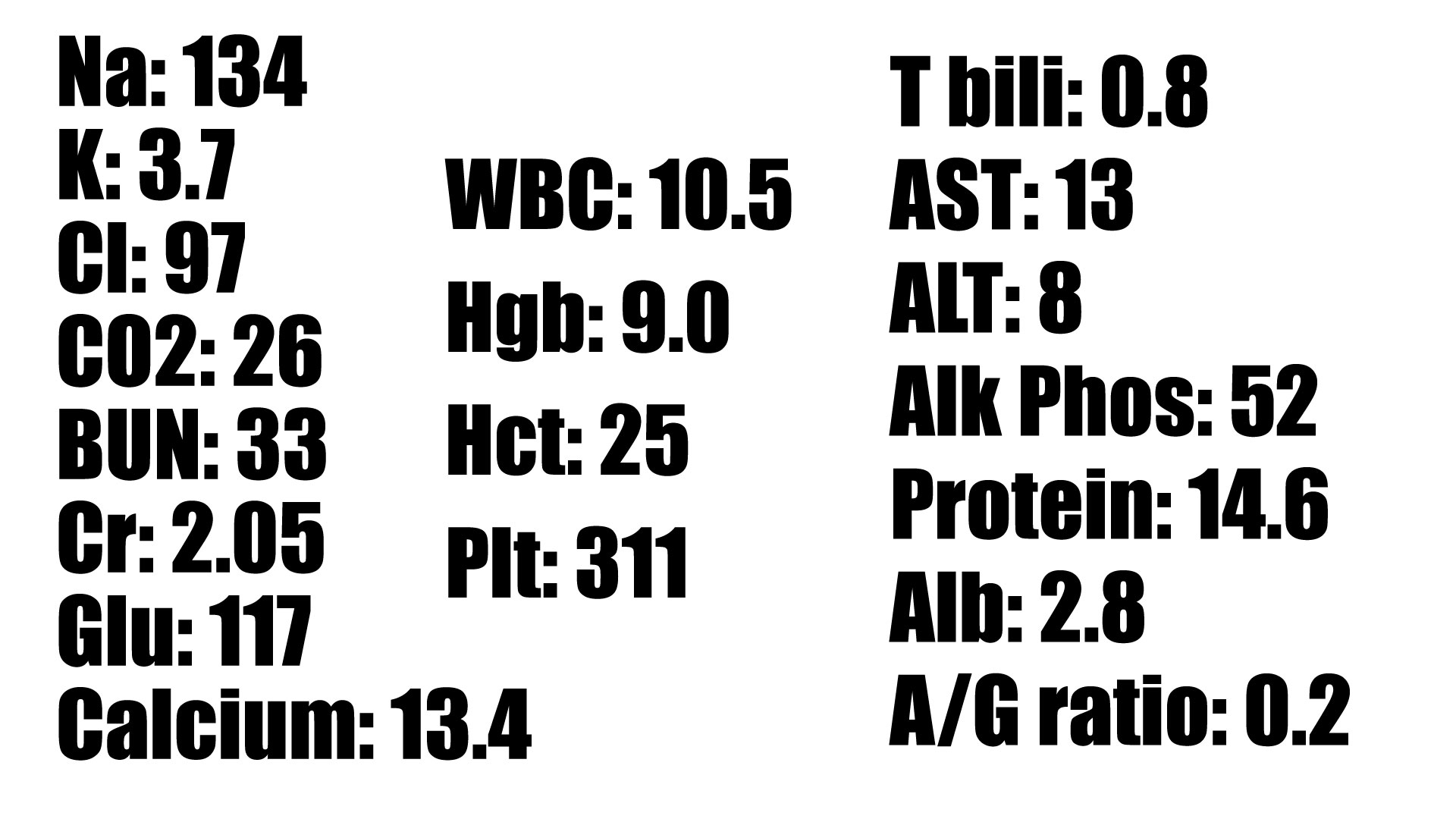
The labs
Any thoughts?
You probably noticed a few things. Specifically, the patient is anemic and has a mildly elevated creatinine. The calcium is elevated, and the protein is very high. As we look even closer, we also notice that the albumin is low. Indeed the A/G ratio (a lab we ED doctors rarely notice) is very low. From a clinical standpoint, let’s also not forget that the patient sought care in the first place for back pain.

Though it is not exactly “diagnostic criteria,” CRAB is the acronym for common presenting signs of multiple myeloma. The presence of these findings is what moves a diagnosis from “smoldering” to “active” multiple myeloma. The discussion that follows is geared towards emergency medicine residents and may seem elementary to people who do this more often. So be it.
What is multiple myeloma?
Multiple myeloma is a cancer of plasma cells. Recall that plasma cells come from B lymphocytes and are the cells that make antibodies, which are proteins. Every plasma cell makes one specific antibody, and in this case a clone of one particular plasma cell divides unchecked. Those clones release a pathological amount of that single antibody.

What’s the bottom line on these labs?
The real finding is the protein. Under normal circumstances, albumin makes up the majority of the serum protein. In this case, however, notice that the total protein is very high, and the albumin is low. That means there must be some protein that is present causing the total to be so much higher than the albumin. That brings up the question alluded to at the outset:
What should the next test be?
We know there is an unidentified extra protein in the blood. Given the CRAB findings in the setting of a protein gap we suspect multiple myeloma. That would mean the extra protein is an immunoglobulin. To sort it out, the next test is a serum protein electrophoresis (SPEP).
Serum proteins are broadly divided into albumin and globulins. The A/G (albumin/globulin) ratio presented on a comprehensive metabolic panel expresses the relationship between the two. Albumin should comprise the largest part of the total, so a normal ratio is greater than 1. When serum is subjected to electrophoresis, the large charged molecules (proteins) move across the medium at different speeds determined by their weight and charge. The result is a separation into five clusters: albumin, alpha-1 globulin, alpha-2 globulin, beta globulin, and gamma globulin. The results are often displayed graphically.
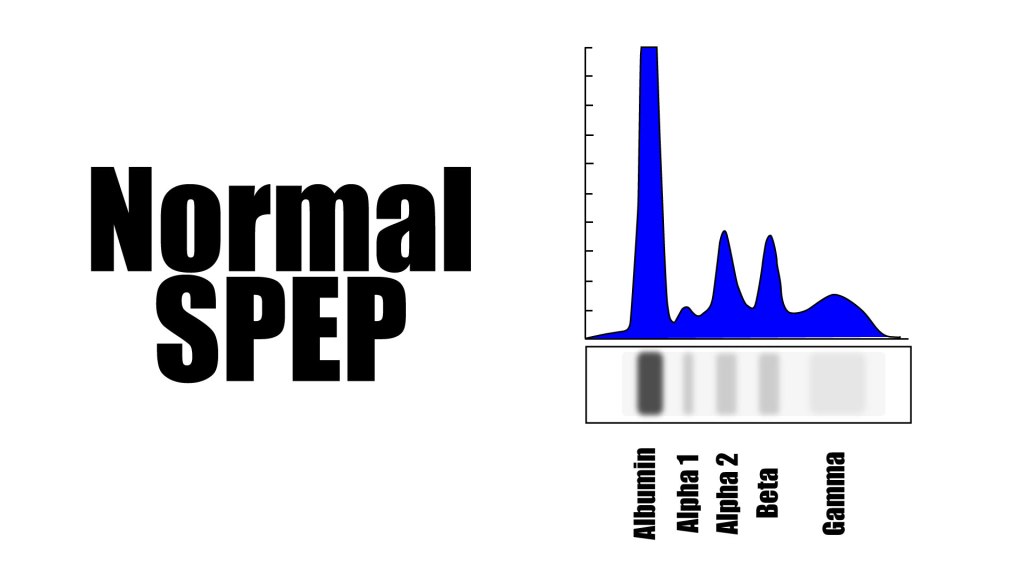
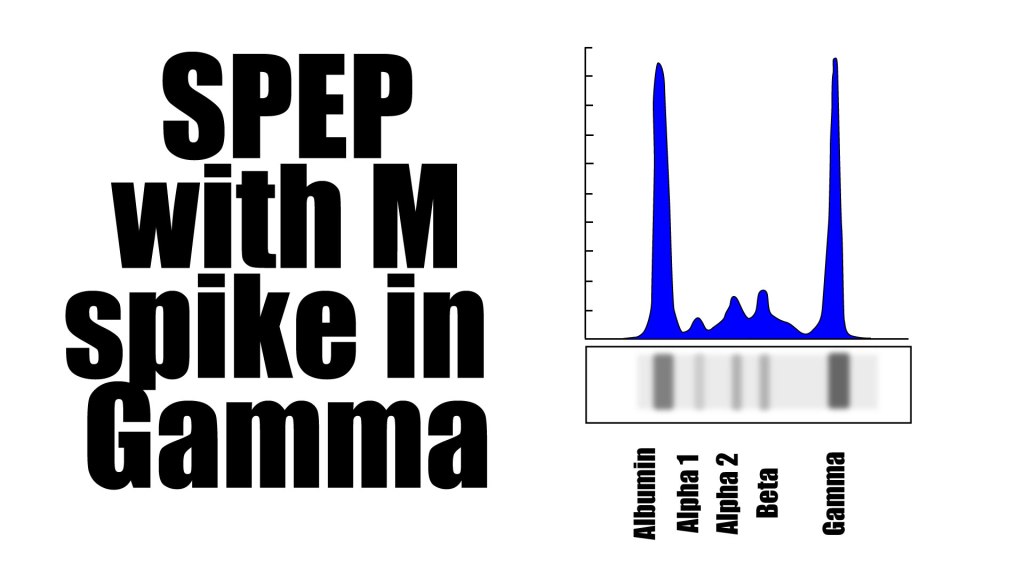
The non-albumin clusters are collectively referred to as “serum globulins.” Immunoglobulins fall into the gamma cluster. The SPEP of a patient with multiple myeloma would show a large spike in the gamma region – the so called “M spike” (M for monoclonal). When you consider that multiple myeloma results from clones of a single plasma cell secreting a protein that is visible in the gamma cluster on SPEP, it becomes clear why it is referred to as a “monoclonal gammopathy.”
Of course, the SPEP doesn’t answer every question. It doesn’t tell you the specific identity of the abnormal protein. You need a few other tests to find the details of the paraprotein (the thing that makes up the M spike). Those include urine protein electrophoresis (UPEP), free light chains, and immunofixation. These tests determine the type of antibody (IgA, IgD, IgE, IgG, IgM) and the type of light chain (kappa or lambda). Skeletal surveys and bone marrow biopsies are essential as well.
What was our patient’s SPEP?

The immunofixation showed that the paraprotein was IgG and the free light chains showed kappa. So, this patient did turn out to have multiple myeloma of the IgG kappa variety.
Let’s Bring it Home
We are very comfortable with an anion gap. A bigger than expected difference between the positive and negative charges means there must be an unmeasured ion in the serum. We then go about figuring out what that unmeasured ion is. The same thought process can be applied to a protein gap. If the total goes up but the albumin doesn’t, there must be something there that isn’t supposed to be. If you find that scenario, the SPEP can help sort it out. Presence of CRAB criteria should set off alarms in your mind to look for that protein. For example, we commonly order basic metabolic panels in the ED, which do not include the protein and albumin levels. Noticing CRAB criteria in the right patient should clue you in to add the hepatic function panel.
Admittedly, this does lean towards the internal medicine side of emergency medicine. SPEP is a send out lab at our hospital, so you wouldn’t have the results even if you were interested enough to send the test. You could certainly get through every ED shift of your career without knowing much about SPEP. However, part of the fun of emergency medicine is getting to dip your toe into the waters of everyone else’s specialty. This isn’t something you will come across every day, but on those rare occasions you can flex your mental muscles and expedite someone’s diagnosis. That’s a win.
