A 45 year-old man presents by EMS after a VF arrest. On arrival at the ED he has a pulse. An ECG shows an anterior STEMI. The cath lab is activated and the cardiologist is en route. While waiting for the cavalry to arrive, you ultrasound his heart and strike gold.
In the setting of an acute myocardial infarction, the segment of myocardium that is supplied by the occluded vessel may not contract during systole. This can be seen on echocardiogram and is called a regional wall motion abnormality. If the occluded vessel (and therefore the affected segment of myocardium) is large enough, we might be able to see the phenomenon on point-of-care ultrasound. The parasternal short axis view in particular is a convenient place to look for this finding.

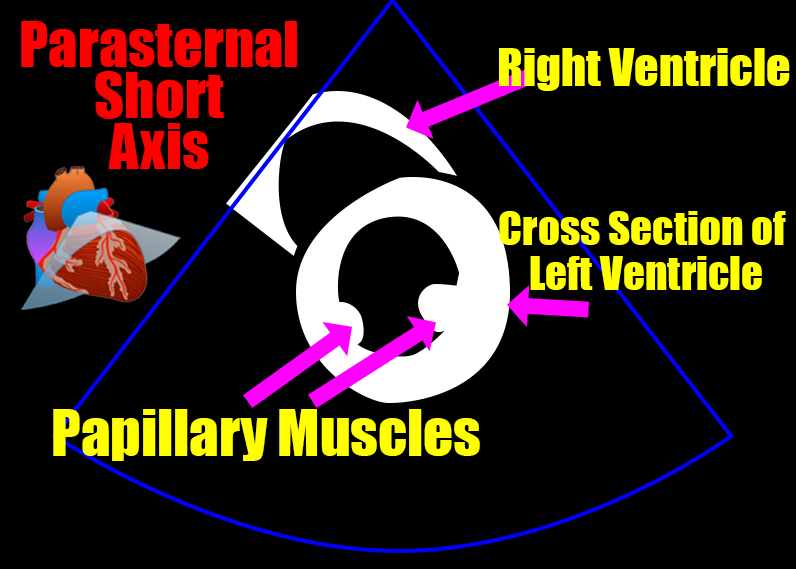
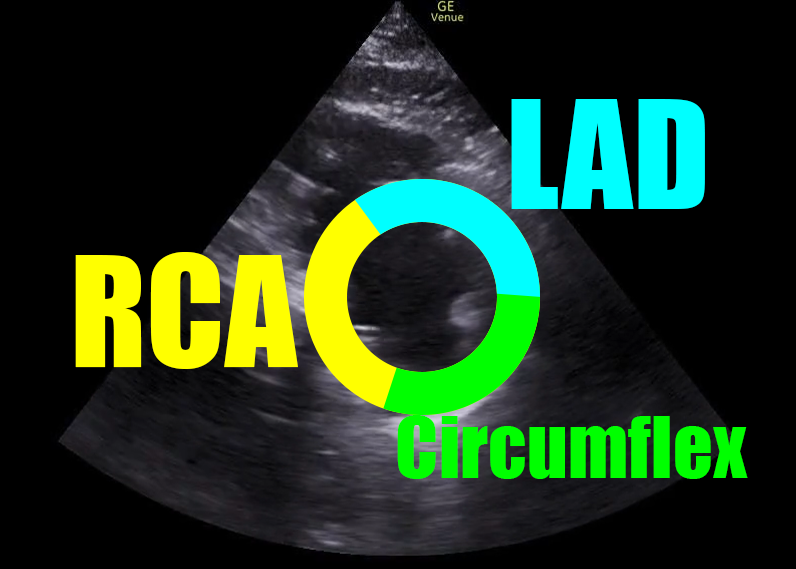
The parasternal short axis view at the level of the papillary muscles shows a segment of the left ventricle that includes territory supplied by all three of the coronary arteries. Here is a crude schematic of those vascular territories.
In a normal heart, the muscle of the left ventricle will contract and all segments will move toward an imaginary center point. It should look like the following image:
Back to our case
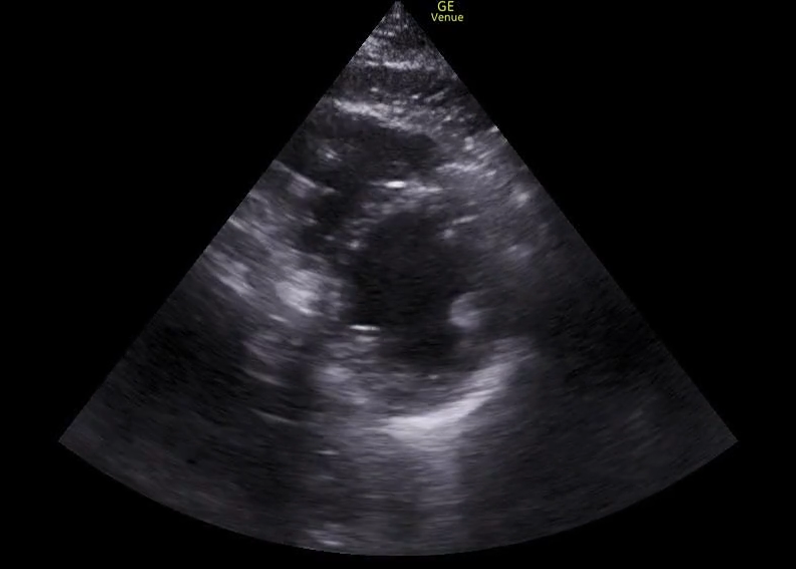
The following images (ECG and parasternal short axis view of the heart) were obtained on our patient immediately following ROSC.
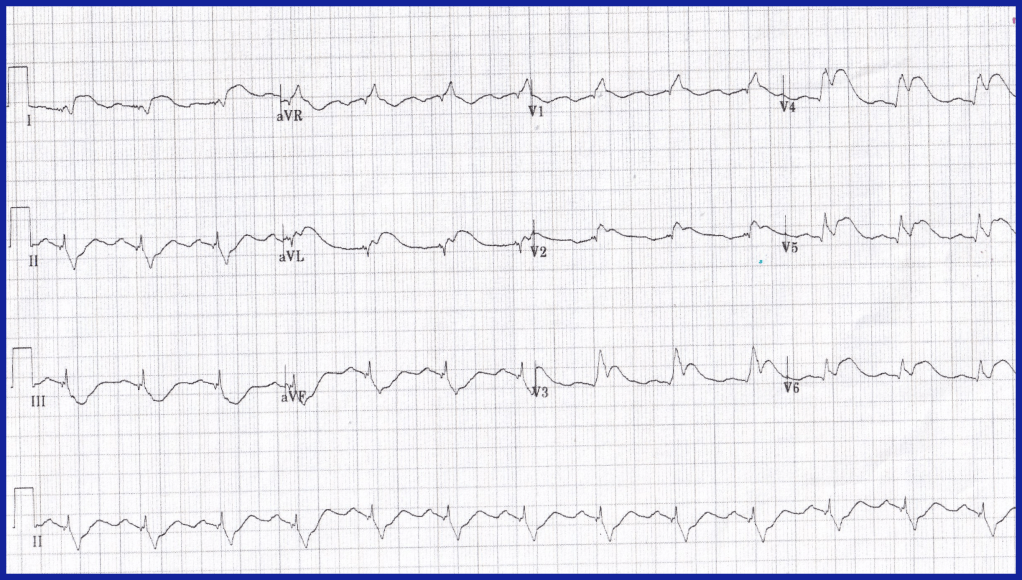
The ECG shows ST segment elevation in the anterior leads, and the ultrasound shows an akinetic segment in the distribution of the LAD. This is the regional wall motion abnormality. The image below illustrates the finding. The heart cath confirmed a total occlusion of the LAD.
Cardiologists use this finding both diagnositically and prognostically. A comprehensive echocardiogram would look for RWMA on more than this one view and there is more subtlety than this very simplified approach allows for. However, there are times when this becomes low-hanging fruit that can be found on point-of-care ultrasound. Happy scanning.
