There are some mistakes that learners commonly make as they are getting the hang of lower extremity DVT ultrasound. Here are some that I see them make when imaging the femoral vein:
- Mistaking the greater saphenous vein for the femoral vein
- Having the probe too distally and not seeing the point where the saphenous joins the common femoral vein
- Finding an image of the femoral vein and thinking it is the common femoral vein
- Not recognizing that they did not actually see the deep femoral vein
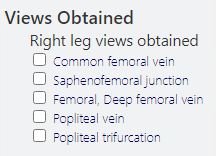
- Checking boxes in the “Views Obtained” section of their Qpath worksheet of images they did not actually obtain. Sometimes this is clerical; other times this represents a knowledge gap.
These problems are easy enough to correct.
- Remember that deep veins have arteries that run parallel to them. If there is no accompanying artery – you aren’t seeing a deep vein. (In this case, you are probably seeing the saphenous.)
- You often need to have the probe slightly more proximal than is comfortable to find the saphenous branch point. Learners often don’t appreciate how ‘friendly’ you have to get with the patient to find this view. Frankly, most of the missteps in imaging the veins of the proximal lower extremity are due to starting the scan too distally – i.e. below the saphenofemoral junction.
- Understand the nomenclature. The “common femoral vein” is above the bifurcation into the “deep femoral vein” and “femoral vein.” It feels like the “femoral vein” should be called the “superficial femoral vein” because it’s counterpart is the “deep femoral vein.” However, since that would put the word “superficial” in the name of what is a deep vein, it is simply called the “femoral vein.”
- The deep femoral vein is a short vessel and can be difficult to see. If you don’t see it, you don’t see it. Luckily, it being short means it is very unusual – though not impossible – to have a DVT isolated to the deep femoral vein.
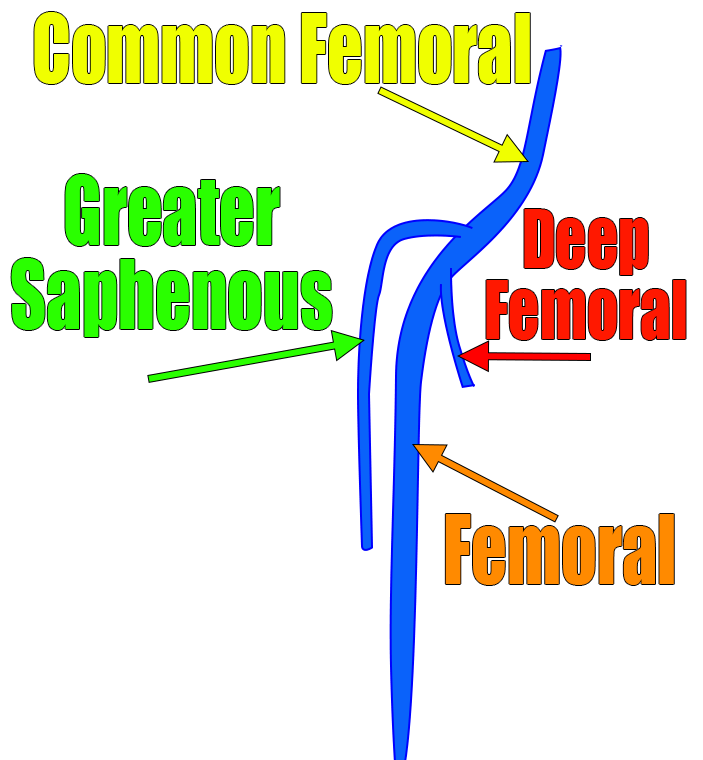
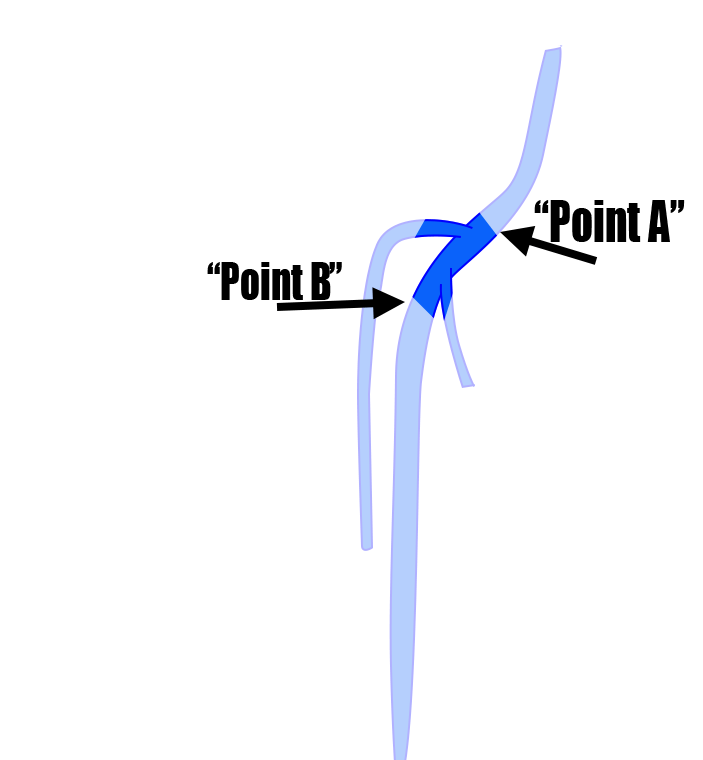
Here we see the anatomy. The point where the saphenous branches from the common femoral vein is the site where blood flow is most turbid. This is very often the site of DVT formation. It is essential to include that point in your study – particularly if you are doing a limited two point compression study. Below is a clip of an ultrasound with a linear probe moving from point A to point B as depicted above. Both left and right are the same clip; the right has labels.
Maybe that clears up some confusion. Maybe you didn’t even realize that you were confused. Either way, as you are learning, be meticulous and find the common femoral vein, saphenous vein, femoral vein and deep femoral vein. Once you see it a few times, you won’t forget it.
**No, this is not the whole story on how to do a DVT scan. But, it is an important part. I suggest you learn it.**
