
Dr. Simmons (by way of the comments on the prior post) has the right answer. This is not a STEMI. As you will recall, not everything with ST elevation is a STEMI. The differential also includes a normal finding in:
- left bundle branch block
- left ventricular hypertrophy
- benign early repolarization
- ventricular paced rhythms
- left ventricular aneurysm
That list is a good one to memorize; but while we are here, lets remind ourselves what a left bundle branch block looks like.
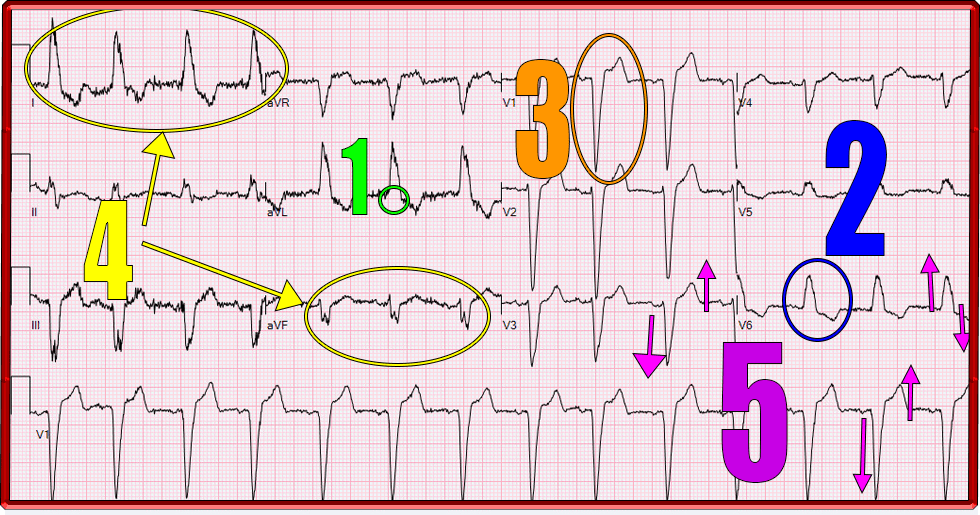
If you’ve only read Dr. Dubin’s book, your lookout for a LBBB ends with looking for an R-R’ in leads V5 and V6. Indeed, you do see a flattening of the R wave in V5 here that you could call R-R’. However, there are some other very classic LBBB findings that we see. From the top:
- QRS duration > 0.12 sec (three small boxes)
- Broad R wave in V5/V6, I, and aVL (sometimes called ‘slurred’ or ‘clumsy’ and may be ‘notched’)(1)
- Deep S wave in V1(2) (and often V2-V4 as seen here)
- Left axis deviation [seen commonly, but not ‘necessarily’ and is not technically part of any diagnostic requirements] (3)
- T waves and ST changes “discordant” to the main vector of the QRS complex [abnormal depolarization is associated with abnormal repolarization]
- In other words, if an S wave is the dominant QRS vector (as is the case in lead V2 here), the T wave will be positive (i.e. opposite of an S wave which by definition is a negative deflection) and ST segment elevation can occur. Elevation in this case would be opposite or “discordant” to the S wave and is considered a normal finding. Any “concordant” ST segment change would be pathologic and concerning for an acute MI – as would “excessive” discordant ST segment elevation (i.e. > 25% of the magnitude of the involved S wave). (4,5)
- [just for laughs, next time you look at a normal EKG – take a moment to notice that the T waves are concordant to the dominant vector of the QRS complex.]
Take home points:
- This is an example of one of the times STE is not a STEMI
- Remember all of the features of a LBBB. It’s on the differential for wide QRS, T wave inversions, ST elevations, and Left Axis deviations.
References:
- Francia P, Balla C, Paneni F, Volpe M. Left bundle-branch block–pathophysiology, prognosis, and clinical management. Clin Cardiol. 2007 Mar;30(3):110-5. doi: 10.1002/clc.20034. PMID: 17385703; PMCID: PMC6653265.
- Nikoo MH, Aslani A, Jorat MV. LBBB: State-of-the-Art Criteria. Int Cardiovasc Res J. 2013 Jun;7(2):39-40. Epub 2013 Jun 1. PMID: 24757618; PMCID: PMC3987432.
- Surawicz B, Childers R, Deal BJ, Gettes LS, Bailey JJ, Gorgels A, Hancock EW, Josephson M, Kligfield P, Kors JA, Macfarlane P, Mason JW, Mirvis DM, Okin P, Pahlm O, Rautaharju PM, van Herpen G, Wagner GS, Wellens H; American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; American College of Cardiology Foundation; Heart Rhythm Society. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009 Mar 17;53(11):976-81. doi: 10.1016/j.jacc.2008.12.013. PMID: 19281930.
- Smith SW, Dodd KW, Henry TD, Dvorak DM, Pearce LA. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med. 2012 Dec;60(6):766-76. doi: 10.1016/j.annemergmed.2012.07.119. Epub 2012 Aug 31. Erratum in: Ann Emerg Med. 2013 Oct;62(4):302. PMID: 22939607.
- Meyers HP, Limkakeng AT Jr, Jaffa EJ, Patel A, Theiling BJ, Rezaie SR, Stewart T, Zhuang C, Pera VK, Smith SW. Validation of the modified Sgarbossa criteria for acute coronary occlusion in the setting of left bundle branch block: A retrospective case-control study. Am Heart J. 2015 Dec;170(6):1255-64. doi: 10.1016/j.ahj.2015.09.005. Epub 2015 Sep 24. PMID: 26678648
