Wellens’ syndrome it is. (For completeness sake, Dr. Wellens has an “s” a the end of his name – it is not “Wellen’s syndrome” it is “Wellens’ syndrome.” And, whether one should use the apostrophe or not with an eponymous syndrome is debatable. Some sources omit it completely: “Wellens Syndrome” but not “Wellen syndrome” – I feel better now that that’s off my chest.)

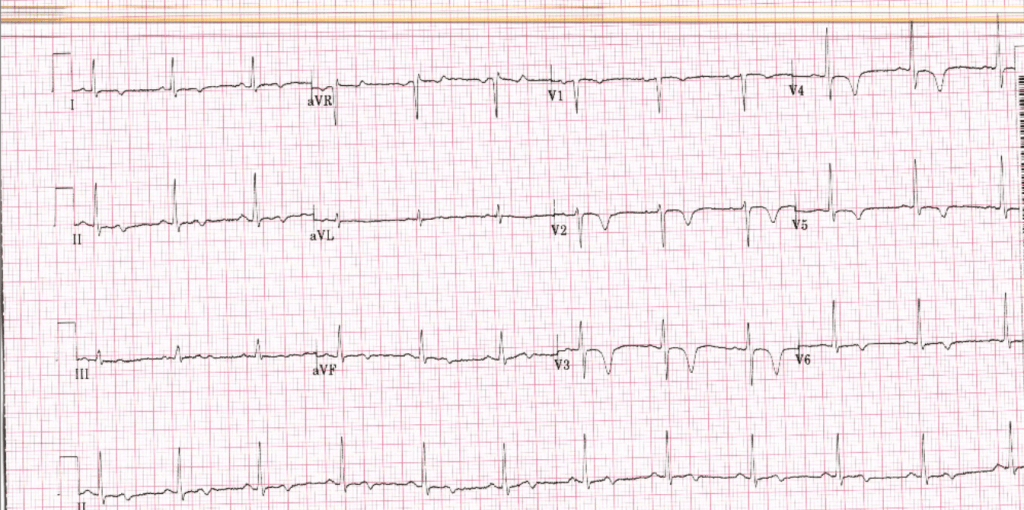
Wellens’ syndrome refers to the phenomenon of a person having had chest pain that generally has resolved at the time of evaluation as well as characteristic findings on the EKG. There are 2 patterns: A and B. Pattern B is what we see in the EKG above and consists of “deep and symmetric” t waves in the anterior leads (specifically V2-V4).
That is opposed to the pattern seen below.
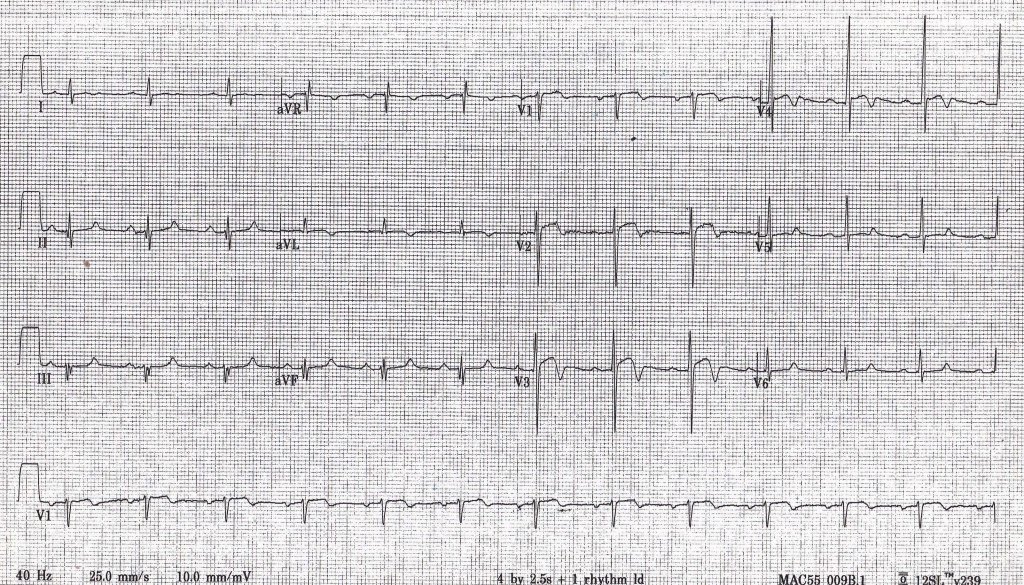
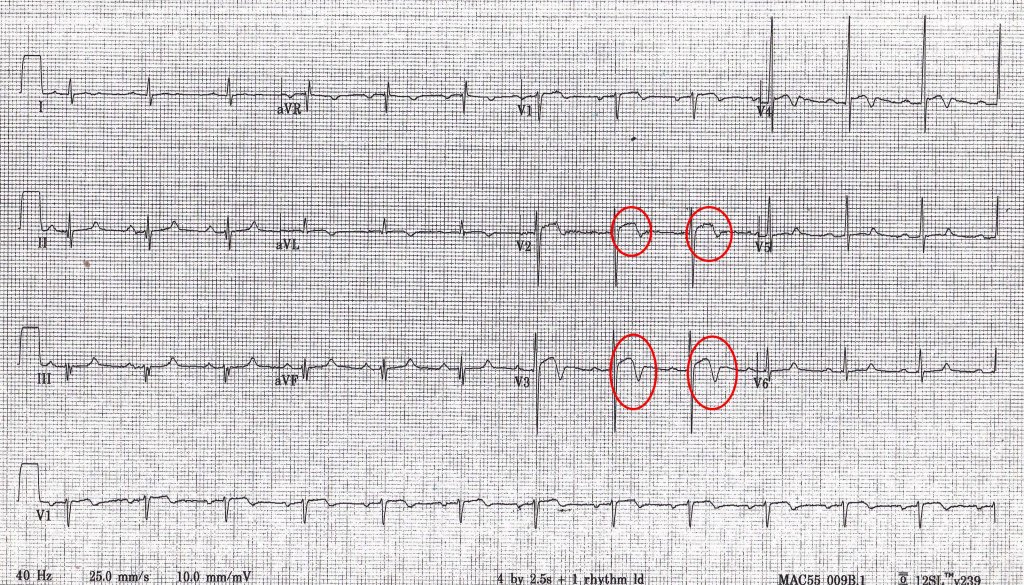
This is an example of a pattern A. It shows biphasic T waves with the initial segment above the isoelectric line and the terminal segment below (inverted, that is).
Pattern B is thought to account for ~ 75% of cases. However, it has been shown (at least in some cases(1)) that the two patterns are on a continuum such that A leads to B over time. So, it you see a pattern B, you may have just missed the pattern A.
These changes are dynamic. In some cases they evolve and develop over the course of the admission(2) without having been present on the initial EKG. They may resolve as well.
The reason this is important is that these changes have been shown to be highly predictive of an advanced stenosis of the LAD, typically the proximal LAD. Progression to an acute MI is very likely over the next several weeks; therefore, this should be evaluated urgently – though not necessarily “emergently.” In other words, you need not activate the cath lab at 3 am for these findings.
In the first case above, the patient’s heart cath showed 95% stenosis of the mid LAD with multi-vessel disease. They were referred for CABG.
The second EKG was from a patient who had been indulging in cocaine. Their heart cath showed no blockages. Their episode of pain and EKG findings were therefore thought to have been due to cocaine induced vasospasm, which likely caused a transient thrombus that self-resolved.
“Dr. Smith’s ECG blog” has several in-depth descriptions of Wellens’ syndrome as does Life in the Fast Lane, if you are interested.
References:
- Dr. Smith’s ECG Blog. https://litfl.com/wellens-syndrome-ecg-library/
- de Zwaan C, Bar FW, Wellens HJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982 Apr;103(4 Pt 2):730-6. PMID: 6121481
